indigoaura
Bluelighter
- Joined
- Jan 4, 2009
- Messages
- 1,707
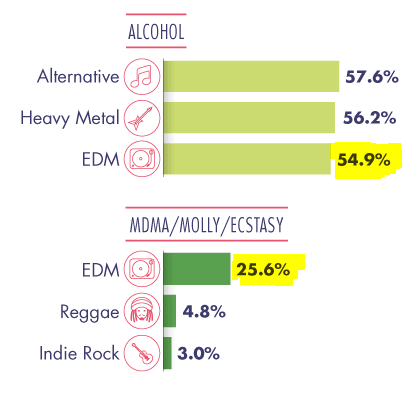
There was some study done a few years ago and the conclusion was that something like 85% of seized "molly" at an ultra music festival one year did not even have trace amounts of MDMA, so i think that even that 25% number of people reporting to have used is way lower.
As for the pupil dilation piece, this, in my opinion, is pointless because there are clearly "meh" product/experiences that cause pupil dilation...
I literally acknowledged this when I posted:
Before the debate ensues, I acknowledge that out of that 25% there will be the typical subset of "bunk" pills in circulation where the user is getting something like meth or tylenol.
But, also, the article I posted never indicated that the MDMA used was purchased at the rave. Considering the change in culture with the rise of the DW, I would assume more people bring their own product than before.
But none of that changes the fact that I have observed, and Biscuit has observed, and a few other people in the EDM scene have also observed, that those who appear to be on MDMA are few and far between at EDM events. This may simply be due to cultural change, as you believe, and an increase in the number of events, or it could somehow be related to the topic of this thread. I genuinely don't understand why a short observation inspires so much debate, however.
Also, where are you seeing people report meh experiences with pupil dilation? I don't recall a lot of them in this thread.
@Negi
Looks like I misread that 2nd study, my apologies.
Perhaps, in general, I overestimate the number of people who do MDMA. I came of age surrounded by MDMA users. My entire social circle revolved around MDMA. For reasons I won't go into here, I had limited socialization and exposure to the world until I left home at 18. At that point, I immediately fell into the race scene and met my people there. My perception of how common MDMA usage is may be skewed by my own experience.