Why do so many people search for a drug or combo that mimics mdma?
Availability? I would prefer plain ol mdma if I where looking for that experience. New research chemicals are not likely to be any healthier than mdma. Most likely the opposite.
I would have said read the damned thread, but it's 30 pp. nao, so. . .
1. There is availability, particularly for those not properly socially embedded to obtain black market items, particularly
genuine black market items. Whatever Chinese chemist or Canadian reseller may flub a bit on the purity of his wares, but chances are that s/he won't
willfully send inert or alternate agents (although tragic accidents HAVE happened, and people have died).
2. MDMA indeed has some issues. While I would deem it near hedonistically ideal in its profile of monaminergic release, some of its neurotoxicity and hangover syndrome are unique to MDxA. In particular, MDxA can form toxic metabolites unique to the particular molecule. Additionally, MDxA and its metabolites can inhibit tryptophan hydroxylase, exacerbating 5ht depletion, but MDxA can also metabolize to alpha-methyl-dopamine, a dopamine antagonist, contributing to the hangover.
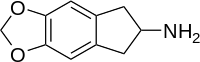
Given the relative safety of MDAI and Methylone (demonstrated by Nichols et al., but of course not in combination), and the possibility that combination of a pure 5ht releaser and a DARI might not present MDMA-like neurotoxicity at all (again, with a tentative basis in research but involving an 'odd' DARI), these sorts of combinations fit into harm reduction.
The problem is the RC stimulants, really. MDPV is known to be comparatively benign physiologically (but kinda doesn't feel so hot). On the other side of the spectrum, mephedrone is likely too cardiotoxic to be used safely. period. Its neurotoxicity is completely unknown, but extremely enduring tolerance to stimulants and empathogens following its overuse presents reason for alarm. Ethcathinone has been demonstrated relatively safe but isn't an ideal stimulant per se (relatively selective NE releaser). And then we have relative unknowns in the middle.
In a magical post-prohibition world, ideal combinations would likely involve methylphenidate, d-amphetamine, or methylone, depending on the user's aim...and possibly IAP rather than MDAI, if some trippiness is desired.
wow, tl;dr.
")
ebola