

-
Neuroscience & Pharmacology Discussion Welcome Guest
Posting Rules Bluelight Rules Recent Journal Articles Chemistry Mega-Thread FREE Chemistry Databases! Self-Education Guide -
N&PD Moderators: Skorpio
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.The Big and Bangin' Pseudo-Advanced Drug Chemistry, Pharmacology and More Thread, V.2
- Thread starter sekio
- Start date
- Status
- Not open for further replies.



Iodjini_dk
Bluelighter
Probably. But to a much lesser extent Id guess. The benzoyl ester is far more bulky and thus resistant to hydrolysis and enzymatic clevage than the methyl ester.Is it possible memantine as an uncompetitive low-affinity NMDA antagonist (that doesn't interfere with regular levels of glutamate agonism) could possibly block or reduce the effects of a partial NMDA receptor agonist like D-Cycloserine? I doubt it, I wanted to read what you folks think. Also, has anyone ever found memantine to block the beneficial recreational/theraputic effects of common psychoactive drugs, in specific speed, LSD, ketamine, GHB, Opiates, MDMA?
Dysphoric
Bluelighter
- Joined
- Feb 3, 2010
- Messages
- 392
How much exactly does your heart rate increase on Meth/Amps?
1.) Lets say a fairly healthy individual took 40mgs of Adderall, how much would their heart rate go up?
2.) And now I want to know what the difference would be if instead they would take Desoxyn at around 20-30mgs, how much of increase?
I would assume Adderall (d-l Amphetamine) is slightly more Cardio-toxic, correct?
I'm curious because that is one thing that gives me anxiety when it comes to drugs, is fast BPM (tachycardia) I have a prescription for Desoxyn, but I've hardly touched it and now that I've started college I want to start taking here and there, around 20-30 mgs. I can handle an increase in BPM, I just don't like too fast, obviously.
Also, I've talked to most of my friends that I've let try Desoxyn before and they said it hardly raised their BPM (vs Adderall), so would Desoxyn hardly touch my BPM at around 20-30mgs?
Also, I'm referring to Oral dosing.Last edited:
23536
Bluelight Crew
Anyone know of any drugs (they don't even need to cross the BBB, just any sort of medically useful molecule) that is hypervalent?
Many sulfur- or phosphorous-containing compounds, like say topiramate, in which the sulfur atom hastentwelve valence electrons:
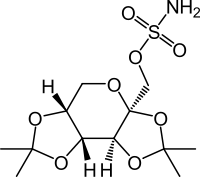
Organophosphates are also hypervalent.
Now how about any hypovalent biologically-active molecules? Organoborides?Last edited:
ebola?
Bluelight Crew
Why don't we yet have a selective dopamine releasing agent? Is this an accident of the array of ligands we're discovered, or is there something about the relevant pharmacology that makes developing such difficult? I would hazard a guess that it's the former, as we have selective releasers of norepinephrine and serotonin...
ebola
Epsilon Alpha
Bluelighter
Well the problem with DAT is how freaking similar it is to NET, in the PFC there aren't even any DAT transporters; NET is responsible for DA uptake there.
Not to mention how DAT is pretty much identical to NET downstream, NE is effectively a slightly more polar version of DA so making a selective releasing agent with traditional SAR pretty much requires making one of those "oily binds to anything amines".
I can go into more detail if you want man.
Peace
-EA
ebola?
Bluelight Crew
Well the problem with DAT is how freaking similar it is to NET
Okay. But we have multiple releasing agents which are selective for NET over DAT...
in the PFC there aren't even any DAT transporters; NET is responsible for DA uptake there.
But yes, we'd need to concede that efflux at NETs entails significant inhibition of reuptake of DA.
Not to mention how DAT is pretty much identical to NET downstream
I don't think that I understand this point. At what point in signaling is the function of DA transporters similar to that of NE transporters? If we're talking about efflux rather than mere transport of the endogenous ligand, does this trend hold?
ebola
Epsilon Alpha
Bluelighter
I don't think that I understand this point. At what point in signaling is the function of DA transporters similar to that of NE transporters? If we're talking about efflux rather than mere transport of the endogenous ligand, does this trend hold?
ebola
Well to my understanding most of the selectivity is conferred by the brain simply having more NE stores and NET transporters, so to reach half maximal activity you need far lower releasing agent concentrations for NE than DA. This is from my pharmacology prof, so it might not follow current research as far as it was the leading theory some years ago.
edit: What I meant for that was catecholamines all share very similar transport/synthesis pathways, so its very difficult to cause selective DA efflux without NE efflux. Though, without a double there are agents more selective for DA vs NE than others. However, as far as agents which bind to random receptors to elicit DA release without NE release then there's a lot of promise for "selective DA releasers"
ebola?
Bluelight Crew
EA said:Well to my understanding most of the selectivity is conferred by the brain simply having more NE stores and NET transporters, so to reach half maximal activity you need far lower releasing agent concentrations for NE than DA. This is from my pharmacology prof, so it might not follow current research as far as it was the leading theory some years ago.
Ah. Right. But if you look at the binding affinities themselves, we have agents where the ki for DAT is 2-3 orders of magnitude larger than the ki for NET. Even in an environment where NET and DAT densities are similar, these agents would remain selective for NET. So my question is, why don't we have ligands where the pattern of affinities and efficacies is reversed?
What I meant for that was catecholamines all share very similar transport/synthesis pathways, so its very difficult to cause selective DA efflux without NE efflux.
Gotcha. Yes, here I concur, given (as you note) the role of DA uptake by NET in the pfc and downstream metabolism of DA to NE. However, there are numerous downstream processes where selective efflux at DAT would have vastly different consequences than selective efflux at NET.
Though, without a double there are agents more selective for DA vs NE than others.
However, we don't yet have agents that are selective for DA per se; every known DA releaser actually has a stronger effect at NE.
ebolaSurfing the digital realms of the internet I found an odd analog, that looks like a arylcyclohexamine analog with a structure best described as being 'in-between' that of Ketamine and Methoxetamine.
It looks like this:
http://f69.myupload.dk/getfile/1122584H-qYXQ3B (click the link)
Chemsketch printed the assumed IUPAC name below, 2-(3-methoxyphenyl)-2-(methylamino)cyclohexanone
After researching a little bit, I have yet to find any data on this.
The site that held it touted it as an "NMDA receptor antagonist and dopamine reuptake inhibitor", which sounds plausible looking at it's close relatives, but hardly verifiable unless there's some hard data to rely on.
It got me curious - so, does anyone recognize this?
I'm dying for some data and/or SAR")
For reference:
Ketamine structure:
http://f69.myupload.dk/getfile/1TskcL3i_
Methoxetamine structure:
https://upload.wikimedia.org/wikipedia/commons/thumb/0/03/Methoxetamine.png/285px-Methoxetamine.png
Thanks
ebola?
Bluelight Crew
Epsilon Alpha
Bluelighter
So this is during a coffee break before a lab so bear with:Ah. Right. But if you look at the binding affinities themselves, we have agents where the ki for DAT is 2-3 orders of magnitude larger than the ki for NET. Even in an environment where NET and DAT densities are similar, these agents would remain selective for NET. So my question is, why don't we have ligands where the pattern of affinities and efficacies is reversed?
Gotcha. Yes, here I concur, given (as you note) the role of DA uptake by NET in the pfc and downstream metabolism of DA to NE. However, there are numerous downstream processes where selective efflux at DAT would have vastly different consequences than selective efflux at NET.
However, we don't yet have agents that are selective for DA per se; every known DA releaser actually has a stronger effect at NE.
ebola
Well most of the problem comes from the fact that using traditional SAR, as things become more selective for DAT vs NET it also starts to bind to other things, for example meth vs regular amp. DAT just loves those oily mofo's.
But what I was getting at is the PKC mediated releasing action really isn't that different for NE vs DA, so using the traditional amphetamine MOA isn't ever really going to give you a greater DA/NE ratio. However, for reuptake inhibitors or things that bind to things like 5ht3 or NAChR there is a strong possibility for making a "selective" indirect DA agonist.
I'll post more when I have more time.
Wouldn't it be "2-keto-3-MeO-PCE" with a methylamine rather than ethylamine?
At this point, the nomenclature becomes almost as lengthy as the IUPAC name!
ebola?
Bluelight Crew
My mistake.
...
EA said:Well most of the problem comes from the fact that using traditional SAR, as things become more selective for DAT vs NET it also starts to bind to other things, for example meth vs regular amp. DAT just loves those oily mofo's.
Ah. This was the piece of the puzzle that I was missing. Still, to my knowledge, we don't even have a DA releaser that is promiscuous at other sites but with negligible affinity for NET.
But what I was getting at is the PKC mediated releasing action really isn't that different for NE vs DA, so using the traditional amphetamine MOA isn't ever really going to give you a greater DA/NE ratio.
Aha! Another piece of the puzzle that I didn't understand. So amphetamine-like efflux is achieved by the exogenous ligand inducing PKC to phosphorylate the transporter (by binding to PKC, changing its conformational form?). Okay, so if this mechanism is fundamentally similar whether we're talking about DAT or NET, why do releasers have any selectivity at all? Are there different isoforms of PKC present proximate to different transporters?
ebola
Epsilon Alpha
Bluelighter
My mistake.
Aha! Another piece of the puzzle that I didn't understand. So amphetamine-like efflux is achieved by the exogenous ligand inducing PKC to phosphorylate the transporter (by binding to PKC, changing its conformational form?). Okay, so if this mechanism is fundamentally similar whether we're talking about DAT or NET, why do releasers have any selectivity at all? Are there different isoforms of PKC present proximate to different transporters?
ebola
An excellent question! Part of the answer comes back to the fact that there is just more NE than DA in the brain period, but I don't know about isoforms I might check it out if I ever see the other side of midterm mountain =/
But, as far as transporter reversal goes there is a ton of evidence implicating PKC as well as many other receptors. But, PKC is what finally phosphorylates the transporter.
Captain.Heroin
Bluelight Crew
How much exactly does your heart rate increase on Meth/Amps?
Dose dependent. Conservative dosages will barely effect it, higher dosages causing concerns of heart failure.helium-4
Bluelight Crew
one of the samples was independently tested.
the more potent one was the one that was independently verified. the less potent one is the one with the vendor crying up and down in the thread that his stuff must be 99.9% pure.
i think i've heard enough lol, thanks guys
the stuff that was third party tested was originally sold as JTE-907 btw. the trip reports made a lot more sense once the lab results came back. glad i stayed away from that one until it got lab confirmed.... UR-144 did end up being pretty nice though.
Do you have a report of the UR-144 any where, or can you describe you're experience I'm getting some in this week and really struggling to find much info- Status
- Not open for further replies.
")