izo
Bluelighter
MT-45
this was not bad at all at 200mg, a solid opioid, as good as tilidine easily.


N&PD Moderators: Skorpio
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
Quinaldine opioids
![]()
izo
Bluelighter
MT-45
this was not bad at all at 200mg, a solid opioid, as good as tilidine easily.
![]()


![]()
Fertile
Bluelighter
As far as I can see, the SAR of opioids is straight out of Alice through the looking glass, so many different compound exhibit opioid activity.
They can all be reconciled. Only today I realised that the reason why 14-methoxymetopon is so potent is that the methoxymerhyl moiety overlays the 4-methoxymethyl of sufentanil.... which is a mixed mu/delta ligand.
The mu/delta ligands seem to represent at once the most potent and the highest TI. Who KNOWS if they are of any interest as an RC. I've read that the effects of sufentanil are much line fentanyl, but not from a reliable source or with any reference. If I found an experience of Sulfenta (sulfentanil) then I would be interested.
The other approach is to go for selective NOP ligands. Janssen accidentally found some but all he did was test analgesia in animal models. Later research shows them to be the most potent class of opioid analgesic but the chemistry is REALLY complex.
I found a paper which used 20 MOP, DOP & KOP ligands and searched for key electronic features (3D QSAR). The MOST potent by far actually turned out to be a NOP selective ligand (but the NOP receptor had not been found at the time). In fact, their are so few known ligands that 3DQSAR is not possible.
It could make a huge difference for those suffering chronic sever pain. I have it, so I do have a vested interest.
Last edited:
![]()
izo
Bluelighter
any info about these mainly delta selective piperazine opioids? guess they are not that interesting from a recreational point of view.
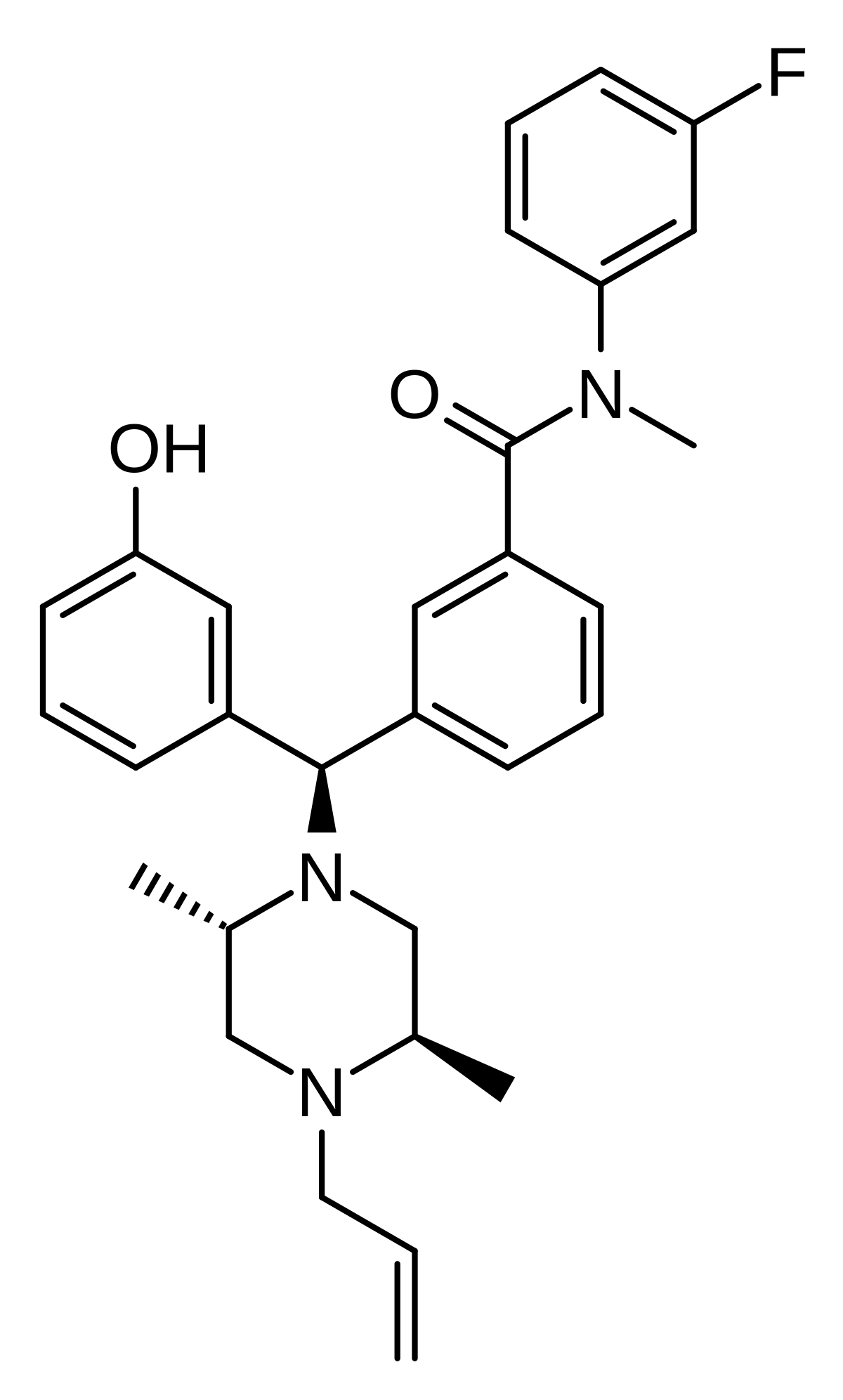
DPI-3290 - Wikipedia
en.wikipedia.org
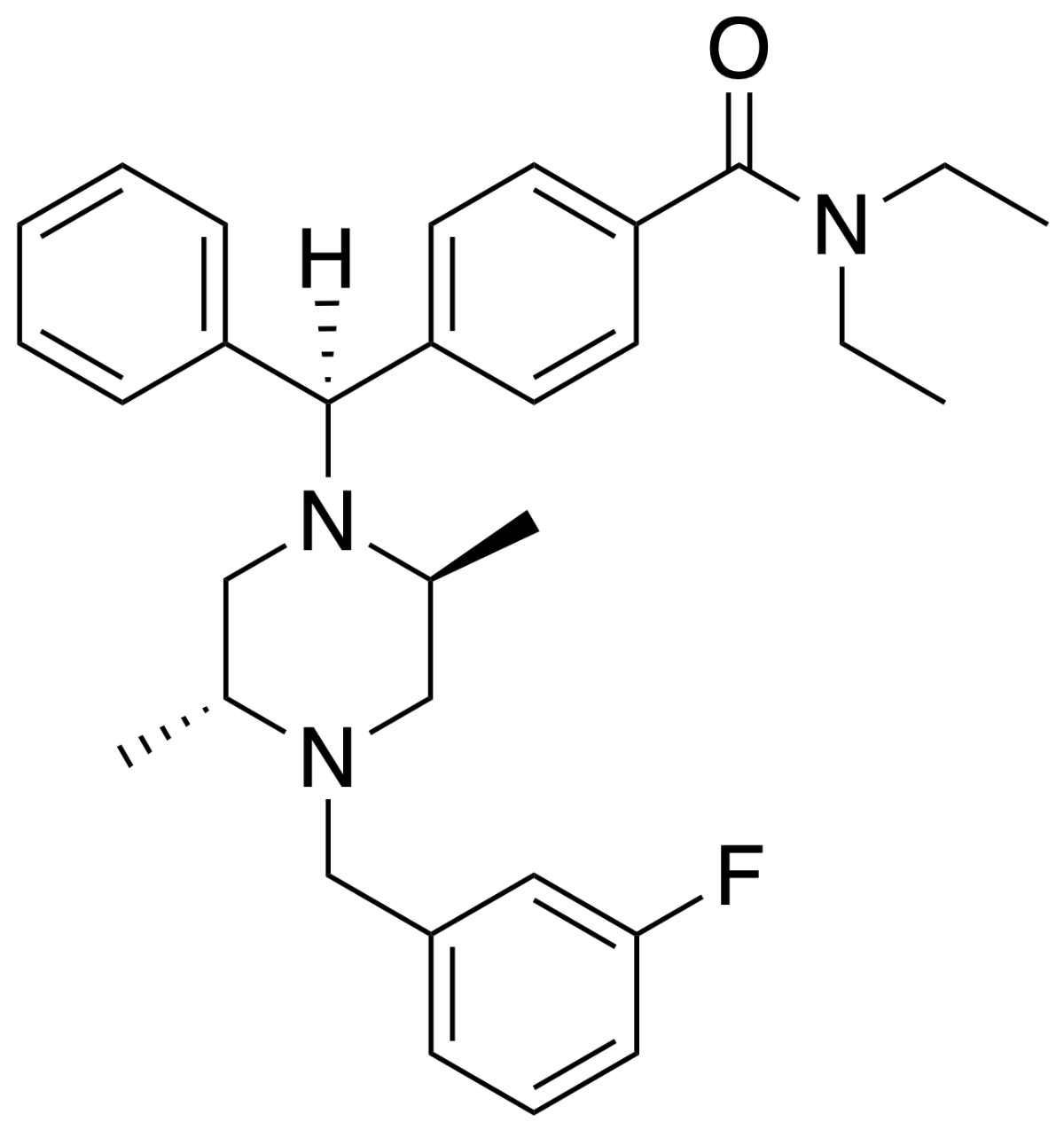
DPI-221 - Wikipedia
en.wikipedia.org
![]()
Fertile
Bluelighter
I wish I could find that 3D QSAR paper. They took 20 MOR, 20 KOR and 20 DOR ligands, calculated affinity and then looked for key moieties. It's amazing that MOR ligands have only 5 key features (the others have 6). A ligand need not have all of the features, but being rigid and having more key moieties increases activity.
![]()
AlsoTapered
Bluelighter
The references to all of the opioids mentioned are not Horlinked in the Useful neuroscience/pharmacology threads thread.
![]()
AlsoTapered
Bluelighter
As far as I can see, the SAR of opioids is straight out of Alice through the looking glass, so many different compound exhibit opioid activity.
There is a Ph.D. thesis, by an Indian guy, about DAT inhibitors etc. that is very interesting reading 
You get a feel. I happened upon nexeridine and while no data was provided, I divined it was an opioid right away. I do NOT consider this to be a skill of value as a genetic trait unless we end up in an AI universe where ANYTHING is available but the buyer has to know what it does... oh, and we are all smack heads.
![]()
polarthedog
Bluelighter
It is a unique drug, the reason why is it not only metabolizes into morphine, it also metabolizes into 6 monoacetyl morphine, and something else too I think but I can’t remember what, and it crosses the blood brain barrier much quicker than morphine would, causing a stronger rush. Users also report less of a histamine release I believe when using heroin versus morphine
It also makes no sense that heroin is considered a unique compound and not a prodrug for morphine
![]()
darvocet21
Bluelighter
Hey polar sup dawg!
It is a unique drug, the reason why is it not only metabolizes into morphine, it also metabolizes into 6 monoacetyl morphine, and something else too I think but I can’t remember what, and it crosses the blood brain barrier much quicker than morphine would, causing a stronger rush. Users also report less of a histamine release I believe when using heroin versus morphine
Morphine is associated with histamine release kind of itching in the veins which is why they will suffuse it into a patient nice and slow
![]()
AlsoTapered
Bluelighter
It is a unique drug, the reason why is it not only metabolizes into morphine, it also metabolizes into 6 monoacetyl morphine, and something else too I think but I can’t remember what, and it crosses the blood brain barrier much quicker than morphine would, causing a stronger rush. Users also report less of a histamine release I believe when using heroin versus morphine
No, there are a few diesters, both symmetrical and asymmetrical that fully substitute for diamorphine (heroin). In fact, 3-propanoyl-6-acetyl morphine was the first 'designer drug' but propanyl, benzyl, nicotinoyl and similar are all essentially identical although just slightly less potent because of the heavier ester moieties.
In fact in the UK dibenzoylmorphine was trialled. I think the reason was that the extra MW meant that it was more or less equipotent with morphine, the idea being, I guess, that it could be directly substituted for morphine - the only difference being a faster onset.
Also, we don't really know much about the 3,14-diacetyl derivative of oxymorphone. Now in related compounds, acetylation of the 14 position increased potency by a factor of 4 although 3 acetylation slightly reduces potency (hence 6MAM being more potent). But it's still going to be about x20 H and if you read reports on oxymorphone, the rush is said to be even more impressive.
I'm not keen on pins. I've never seen a story end well when people wind up IVing drugs.