JohnBoy2000
Bluelighter
- Joined
- May 11, 2016
- Messages
- 2,665
As per the last post in this sub, for the purpose of treating or relieving cognitive fatigue, I have found methamphetamine significantly more effective at a much lower dose, than I have either methylphenidate (which did little to nothing), or amphetamine (which required ridiculous doses for effect and frequent re-dosing for sustained effect).
Of course I've read ad nauseum warnings across bluelight as to the high abuse and addiction potential of this potentially devastating drug.
For this reason I've been particularly prudent with my approach, understanding the remarkable "relief" benefits I've experienced from it and therefore proceeding such to pay particular attention to potential harm and addiction.
Attempting to following FDA approved clinical dosing protocol was the first measure, where it's maximum is conventionally listed as being 25 mg for pharma grade "desoxyn".
As I am using "crystal" purchased on DNM's, I'm unsure of dosing equivalency but for adequate effect over a period of about 8 to 10 hours, I found it necessary to dose up to a maximum of 35 mg (so far).
Additionally to avoid excessive half-life/elimination-time and accompanying insomnia - I'm using nasal (snorting) administration (which I understand also increases bioavailability V digestion).
**
I've used the following link as a generalized guide to dosing, Tmax and half-life per each ROA;
 psychonautwiki.org
psychonautwiki.org
**
Using google scholar to find more in depth dosing information,
https://mn.gov/law-library-stat/archive/urlarchive/a080579.pdf
This information leaflet notes a max daily dose of 60 mg (which is obviously a potentially euphoric dose for an infrequent user).
**
The drugs.com review section gives a series on anecdotal reports on the subjective outcome of conventional stimulants V methaphetamine
 www.drugs.com
www.drugs.com
...... which I was certainly able to relate to given my subjective lack of success with conventional stimulants.
**
And finally I couldn't help but notice,
 journals.lww.com
journals.lww.com
Papers and articles such as this, illustrating supposed neural benefits of neural compromise in cases such as Traumatic-Brain-Injury (TBI).
Of course I've read ad nauseum warnings across bluelight as to the high abuse and addiction potential of this potentially devastating drug.
For this reason I've been particularly prudent with my approach, understanding the remarkable "relief" benefits I've experienced from it and therefore proceeding such to pay particular attention to potential harm and addiction.
(I've dosed it 3 times over the past 2 weeks).
Attempting to following FDA approved clinical dosing protocol was the first measure, where it's maximum is conventionally listed as being 25 mg for pharma grade "desoxyn".
As I am using "crystal" purchased on DNM's, I'm unsure of dosing equivalency but for adequate effect over a period of about 8 to 10 hours, I found it necessary to dose up to a maximum of 35 mg (so far).
Additionally to avoid excessive half-life/elimination-time and accompanying insomnia - I'm using nasal (snorting) administration (which I understand also increases bioavailability V digestion).
**
I've used the following link as a generalized guide to dosing, Tmax and half-life per each ROA;
Methamphetamine
N-Methylamphetamine (also known as Methamphetamine, Ma, Meth, Glass, Ice, Shard, Crank, Tina, T, Tweak, Yaba, Shabu, and Crystal[3]) is a classical stimulant substance of the amphetamine class. It is structurally related to amphetamine, however it crosses the blood-brain barrier more rapidly...
**
Using google scholar to find more in depth dosing information,
https://mn.gov/law-library-stat/archive/urlarchive/a080579.pdf
This information leaflet notes a max daily dose of 60 mg (which is obviously a potentially euphoric dose for an infrequent user).
**
The drugs.com review section gives a series on anecdotal reports on the subjective outcome of conventional stimulants V methaphetamine
Methamphetamine Reviews & Ratings - Drugs.com
Reviews and ratings for Methamphetamine. 79 reviews submitted with a 8.8 average score.
...... which I was certainly able to relate to given my subjective lack of success with conventional stimulants.
**
And finally I couldn't help but notice,
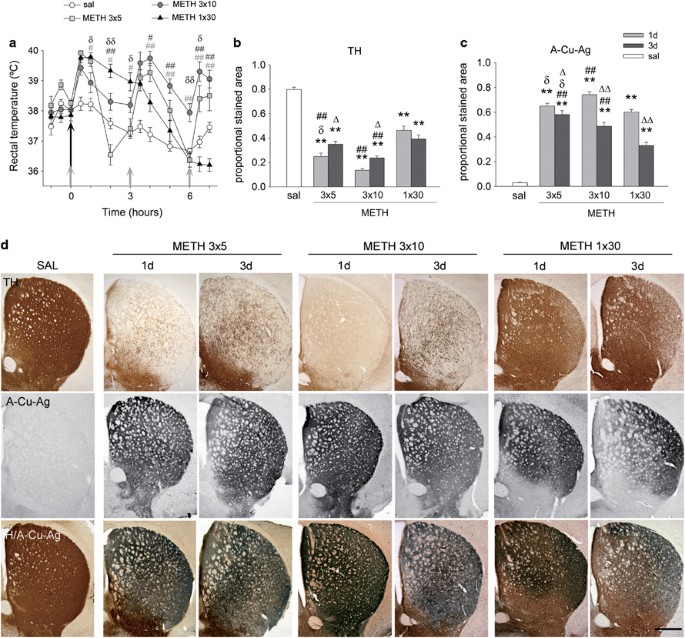
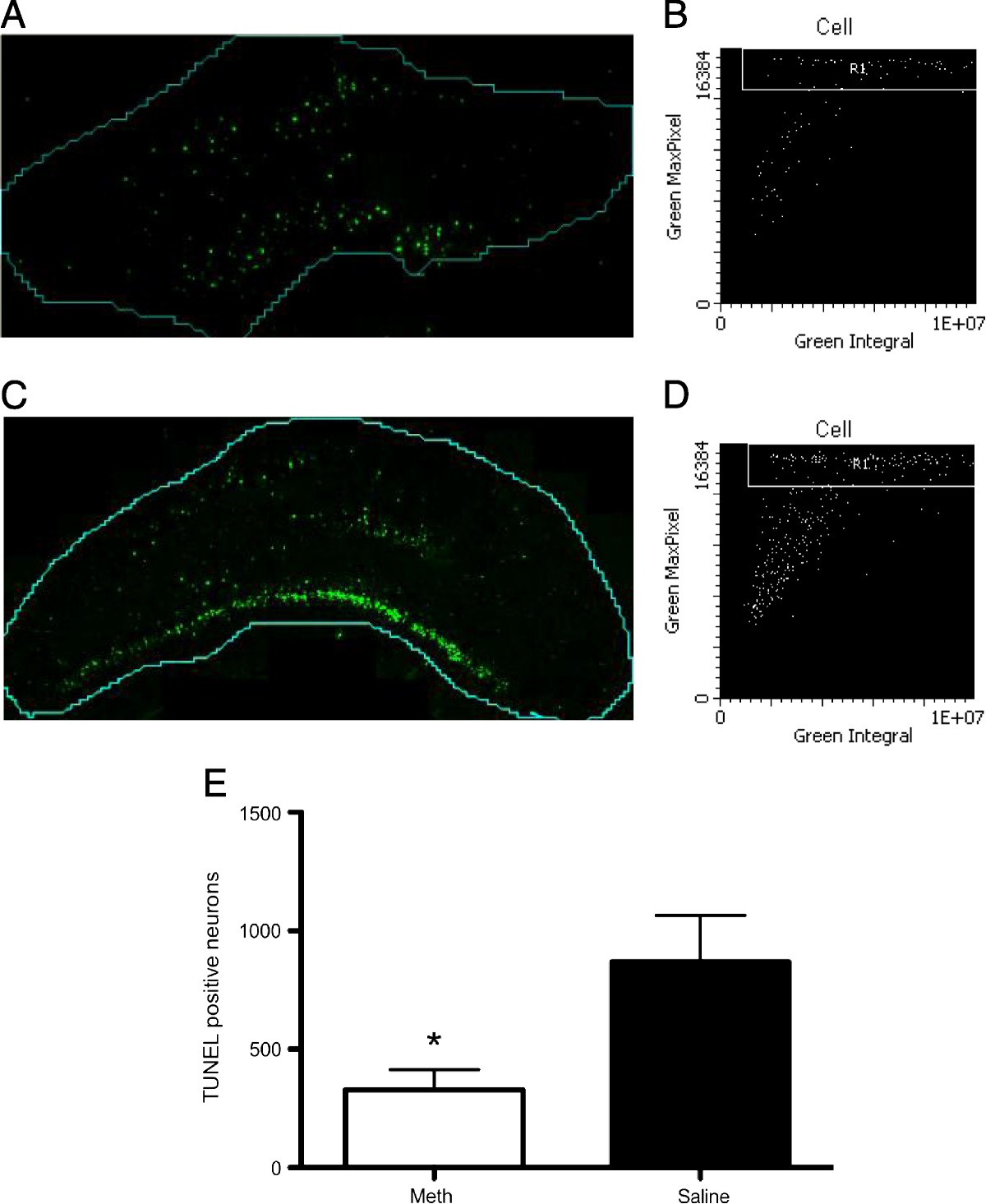
Treatment with low-dose methamphetamine improves behavioral ... : Journal of Trauma and Acute Care Surgery
is finding, we hypothesized that methamphetamine could also prevent neuronal loss and improve functional behavior after severe traumatic brain injury (TBI). METHODS The rat lateral fluid percussion injury model was used to generate severe TBI. Three hours after injury, animals were treated with...
journals.lww.com
Papers and articles such as this, illustrating supposed neural benefits of neural compromise in cases such as Traumatic-Brain-Injury (TBI).
Last edited: