

red22
Bluelighter
- Joined
- Nov 23, 2009
- Messages
- 2,074
A FATAL POISONING WITH LSD
R.R. FYSH, M.C.H. OON, K.N. ROBINSON, R.N. SMITH, P.C. WHITE and M.J. WHITEHOUSE
Metropolitan Police Forensic Science Laboratory, 109 Lambeth Road, London SE1 7LP (U.K.)
(Received January 3, 1985)
(Revision received February 28, 1985)
(Accepted February 28, 1985)
Summary
Radioimmunoassay, high-performance liquid chromatography and capillary gas chromatography-mass spectrometry were used to detect and measure LSD in the first reported case of fatal poisoning by LSD. The levels found in ante-mortem serum and plasma and in post-mortem blood, liver blood and stomach contents are given.
Key words: Fatal LSD poisoning; Toxicological analysis of LSD; Ante- and post-mortem LSD levels.
Introduction
Fatalities associated with lysergide (LSD) are usually due to injuries received whilst under the influence of the drug. In a recent case, however, a 25-year-old male died 16 h after being admitted to hospital, and a Coroner's enquiry concluded, on the basis of the medical and toxicological evidence, that the actual cause of death was poisoning by LSD. This paper describes the toxicological aspects of the case in which LSD was analysed in ante- and post-mortem samples by various techniques.
Ante-mortem serum and plasma and post-mortem blood, liver blood and stomach contents were available for toxicological examination. The samples were analysed quantitatively for LSD by radioimmunoassay (RIA). High-performance liquid chromatography (HPLC) and capillary gas chromatography-mass spectrometry (capillary GC-MS) were used to confirm the presence of LSD and to verify some of the quantitative results.
Routine toxicological examination of the liver was carried out elsewhere prior to submission of the samples to this laboratory; no drugs were detected. RIA of the ante-mortem serum in this laboratory demonstrated the absence of amphetamine [1] and cannabinoids [2], thus LSD was the only drug detected in the case.
Materials and Methods
1. Sample preparation
Samples (100-μl) for RIA were vortexed with methanol (300-μl), allowed to stand for 15—30 min and centrifuged for 2 min (12,000 g). Aliquots (200-μl) of the methanolic supernatants were evaporated to dryness in silanised glass tubes under a stream of air at room temperature and taken up in 0.05 M barbitone buffer (200 μl) (pH 8.6) containing 0.1% w/v bovine serum albumin and 0.1% w/v sodium azide.
Plasma (1.0 ml) for HPLC analysis was mixed with 2 N ammonium hydroxide (100 μl) and extracted with diethyl ether (2 × 3 ml). The extracts were pooled, evaporated to dryness at 60°C under nitrogen in darkness and reconstituted in HPLC eluent (150 μl).
Stomach contents (4.0 g) for HPLC and capillary GC-MS analysis were mixed with concentrated ammonium hydroxide (1.0 ml) and extracted with ether (2 × 3 ml). The extracts were pooled, evaporated to dryness at 60°C under nitrogen in darkness, reconstituted in 0.1 N hydrochloric acid (100 μl) and washed with ether (2 × 200 μl). The acid solution was made alkaline with concentrated ammonium hydroxide (100 μl) and extracted with ether (2 × 3 ml). The extracts were pooled, evaporated to dryness at 60°C under nitrogen in darkness and reconstituted in HPLC eluent (2 ml). This reconstituted extract was analysed by HPLC. For capillary GC-MS analysis, the extract was evaporated to dryness at 60°C under nitrogen in darkness and reconstituted in water (200 μl). The pH was adjusted to 10 with concentrated ammonium hydroxide and the solution was extracted with ether (2 × 3 ml). The extracts were combined, evaporated to dryness at 60°C under nitrogen in darkness and reconstituted in methanol (20 μl).
2. Radioimmunoassay (RIA)
The reconstituted extracts were assayed for LSD by the method of Ratcliffe et al. [3]. The antiserum (provided by courtesy of the Central Research Establishment, Home Office Forensic Science Service) was raised in sheep using an LSD-bovine serum albumin conjugate in which the indolic nitrogen of LSD was linked to the protein.
The recovery of LSD from blood samples spiked at 25 ng/ml was found to be 88% with a coefficient of variation of 14.5% (n = 10). The detection limit of the assay was 2.8 ng/ml (mean response of 24 blank blood extracts plus 3 standard deviations, multiplied by 4 to allow for dilution of the blood samples in preparing the extracts).
3. High-performance liquid chromatography (HPLC)
HPLC was carried out on a 24 cm × 4.9 mm i.d. column of Spherisorb S5W silica (Phase Separations, Queensferry, Clwyd). The eluent was 0.01 M ammonium perchlorate in HPLC-grade methanol adjusted to pH 6.7 with 0.1 M sodium hydroxide in methanol. The flow-rate was 1.0 ml/min. A Fluoromonitor III fluorescence detector fitted with a zinc lamp was used (Laboratory Data Control, Stone, Staffordshire). The excitation wavelength was 308 nm and the emission was measured through a 370—700-nm filter. Injections were made under continuous flow conditions via an injection valve (Negretti and Zambra, Southampton, Hampshire) fitted with a 25-μl loop.
4. Capillary GC-MS
The stomach contents extract was analysed by capillary GC-MS using a Carlo Erba Fractovap Series 4160 GC (Erba Science, Swindon, Wiltshire) coupled to a VG Micromass 12-12F quadrupole MS (VG Masslab, Altrincham, Cheshire). The GC column was a 12-m bonded phase BP-1 capillary (SGE, Milton Keynes, Buckinghamshire) which led directly into the ion source of the MS. The carrier gas was helium at an inlet pressure of 1.3 kg/cm². The injector temperature was 250°C. Splitless injections (0.5 μl) were made and the injection port was vented after 50 s. The column was held at 100°C for 1 min after injection and was then raised to 280°C at approximately 40°C/min. The MS was operated in the electron impact mode with an accelerating voltage of 70 eV. The interface temperature was 250°C and the source temperature was 200°C. Multiple ion detection was used to monitor LSD ions of m/e 323 (molecular ion) and 181.
Results and discussion
LSD was detected by RIA in all the samples. The levels found are given in Table 1 and may include a response to cross-reacting metabolites in addition to unchanged LSD.
Ante-mortem plasma (Fig. 1) and stomach contents extracts were analysed for LSD by HPLC. A peak with a retention identical to that of authentic LSD was detected in each extract. Comparison of the peak heights with those of known concentrations of LSD gave the levels shown in Table 1.
TABLE 1
LSD LEVELS FOUND BY RIA AND HPLC
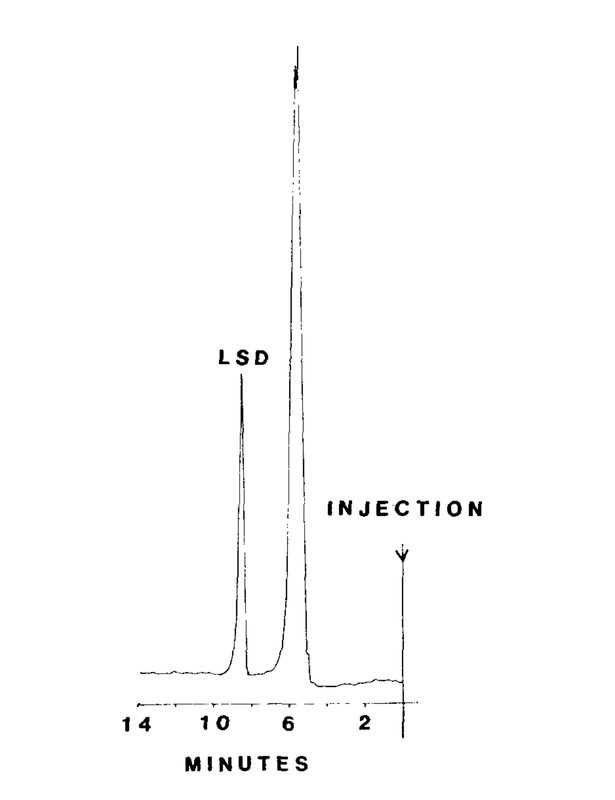
Fig. 1. HPLC of ante-mortem plasma extract. Conditions as described in the text; 25 μl injected. The unlabelled peak (solvent front) is typical of that observed with control samples.
The results compared reasonably well with those obtained by RIA. Coextractives or insufficient sample precluded HPLC analysis of the other samples.
The stomach contents extract was analysed by capillary GC-MS. Ions of m/e 323 and 181 were monitored by multiple ion detection and gave peaks with a retention of 10.0 min. Identical results were obtained with authentic LSD. The other samples were not examined by capillary GC-MS.
It is difficult to assess the significance of the results in Table 1 since no fatal levels of LSD in humans are given in the literature. The highest plasma level of LSD previously found [4] was 9.5 ng/ml, and was the mean plasma level of 5 subjects 5 min after intravenous injection of 2 μg LSD/kg. Individual levels were not given. In the same study, the half-life of LSD in plasma was calculated to be 175 min. In another study [5], 13 subjects were each given 160 μg LSD orally and plasma levels of LSD were measured at intervals up to 5 h. The highest level found in any subject was 8.8 ng/ml after 130 min. The other plasma levels in these studies were generally much lower, as were the plasma levels found in other cases of LSD ingestion [3,6,7]. In one previous case in this laboratory (unpublished results), we found LSD in both blood and stomach contents at levels of 7.6 and 11.6 ng/ml, respectively. In a further five cases in which we found LSD in stomach contents, the blood levels were below the RIA detection limit (2.8 ng/ml). In four cases in which LSD was detected in blood, but stomach contents were not available for analysis, the levels ranged from 4.4 to 8.0 ng/ml. The levels found in the ante-mortem samples in the present case (Table 1) are thus nearly double the highest levels previously found in blood.
References
1 R.N. Smith, Immunoassays in forensic toxicology. In J.S. Oliver (ed.), Forensic Toxicology, Croom Helm, London, 1080, pp. 34—47.
2 B. Law, P.A. Mason, A.C. Moffat and L.J. King, A novel ¹²⁵I-radioimmunoassay for the analysis of Δ⁹-tetrahydrocannabinol and its metabolites in human body fluids. J. Anal. Toxicol., 8 (1984) 14—18.
3 W.A. Ratcliffe, S.M. Fletcher, A.C. Moffat, J.G. Ratcliffe, W.A. Harland and T.E. Levitt, Radioimmunoassay of lysergic acid diethylamide (LSD) in serum and urine using antisera of different specificities. Clin. Chem., 23 (1977) 169—174.
4 G.K. Aghajanian and O.H.L. Bing, Persistence of lysergic acid diethylamide in the plasma of human subjects. Clin. Pharmacol. Ther., 5 (1964) 611—614.
5 D.G. Upshall and D.G. Wailling, The determination of LSD in human plasma following oral administration. Clin. Chim. Acta, 36 (1972) 67—73.
6 B. Widdop, The detection of LSD in biological fluids. Bull. Int. Assoc. Forensic Toxicol., 7 (1971) 6—7.
7 P.J. Twitchett, S.M. Fletcher, A.T. Sullivan and A.C. Moffat, Analysis of LSD in human body fluids by high-performance liquid chromatography, fluorescence spectroscopy and radioimmunoassay. J. Chromatog., 150 (1978) 73—84.
Fysh, R. R. 1985. A fatal poisoning with LSD. Oon, M. C., Robinson, K. N., Smith, R. N., White, P. C., Whitehouse, M. J. Forensic Sci Int, 28(2), 109–13 10.1016/0379-0738(85)90067-2
R.R. FYSH, M.C.H. OON, K.N. ROBINSON, R.N. SMITH, P.C. WHITE and M.J. WHITEHOUSE
Metropolitan Police Forensic Science Laboratory, 109 Lambeth Road, London SE1 7LP (U.K.)
(Received January 3, 1985)
(Revision received February 28, 1985)
(Accepted February 28, 1985)
Summary
Radioimmunoassay, high-performance liquid chromatography and capillary gas chromatography-mass spectrometry were used to detect and measure LSD in the first reported case of fatal poisoning by LSD. The levels found in ante-mortem serum and plasma and in post-mortem blood, liver blood and stomach contents are given.
Key words: Fatal LSD poisoning; Toxicological analysis of LSD; Ante- and post-mortem LSD levels.
Introduction
Fatalities associated with lysergide (LSD) are usually due to injuries received whilst under the influence of the drug. In a recent case, however, a 25-year-old male died 16 h after being admitted to hospital, and a Coroner's enquiry concluded, on the basis of the medical and toxicological evidence, that the actual cause of death was poisoning by LSD. This paper describes the toxicological aspects of the case in which LSD was analysed in ante- and post-mortem samples by various techniques.
Ante-mortem serum and plasma and post-mortem blood, liver blood and stomach contents were available for toxicological examination. The samples were analysed quantitatively for LSD by radioimmunoassay (RIA). High-performance liquid chromatography (HPLC) and capillary gas chromatography-mass spectrometry (capillary GC-MS) were used to confirm the presence of LSD and to verify some of the quantitative results.
Routine toxicological examination of the liver was carried out elsewhere prior to submission of the samples to this laboratory; no drugs were detected. RIA of the ante-mortem serum in this laboratory demonstrated the absence of amphetamine [1] and cannabinoids [2], thus LSD was the only drug detected in the case.
Materials and Methods
1. Sample preparation
Samples (100-μl) for RIA were vortexed with methanol (300-μl), allowed to stand for 15—30 min and centrifuged for 2 min (12,000 g). Aliquots (200-μl) of the methanolic supernatants were evaporated to dryness in silanised glass tubes under a stream of air at room temperature and taken up in 0.05 M barbitone buffer (200 μl) (pH 8.6) containing 0.1% w/v bovine serum albumin and 0.1% w/v sodium azide.
Plasma (1.0 ml) for HPLC analysis was mixed with 2 N ammonium hydroxide (100 μl) and extracted with diethyl ether (2 × 3 ml). The extracts were pooled, evaporated to dryness at 60°C under nitrogen in darkness and reconstituted in HPLC eluent (150 μl).
Stomach contents (4.0 g) for HPLC and capillary GC-MS analysis were mixed with concentrated ammonium hydroxide (1.0 ml) and extracted with ether (2 × 3 ml). The extracts were pooled, evaporated to dryness at 60°C under nitrogen in darkness, reconstituted in 0.1 N hydrochloric acid (100 μl) and washed with ether (2 × 200 μl). The acid solution was made alkaline with concentrated ammonium hydroxide (100 μl) and extracted with ether (2 × 3 ml). The extracts were pooled, evaporated to dryness at 60°C under nitrogen in darkness and reconstituted in HPLC eluent (2 ml). This reconstituted extract was analysed by HPLC. For capillary GC-MS analysis, the extract was evaporated to dryness at 60°C under nitrogen in darkness and reconstituted in water (200 μl). The pH was adjusted to 10 with concentrated ammonium hydroxide and the solution was extracted with ether (2 × 3 ml). The extracts were combined, evaporated to dryness at 60°C under nitrogen in darkness and reconstituted in methanol (20 μl).
2. Radioimmunoassay (RIA)
The reconstituted extracts were assayed for LSD by the method of Ratcliffe et al. [3]. The antiserum (provided by courtesy of the Central Research Establishment, Home Office Forensic Science Service) was raised in sheep using an LSD-bovine serum albumin conjugate in which the indolic nitrogen of LSD was linked to the protein.
The recovery of LSD from blood samples spiked at 25 ng/ml was found to be 88% with a coefficient of variation of 14.5% (n = 10). The detection limit of the assay was 2.8 ng/ml (mean response of 24 blank blood extracts plus 3 standard deviations, multiplied by 4 to allow for dilution of the blood samples in preparing the extracts).
3. High-performance liquid chromatography (HPLC)
HPLC was carried out on a 24 cm × 4.9 mm i.d. column of Spherisorb S5W silica (Phase Separations, Queensferry, Clwyd). The eluent was 0.01 M ammonium perchlorate in HPLC-grade methanol adjusted to pH 6.7 with 0.1 M sodium hydroxide in methanol. The flow-rate was 1.0 ml/min. A Fluoromonitor III fluorescence detector fitted with a zinc lamp was used (Laboratory Data Control, Stone, Staffordshire). The excitation wavelength was 308 nm and the emission was measured through a 370—700-nm filter. Injections were made under continuous flow conditions via an injection valve (Negretti and Zambra, Southampton, Hampshire) fitted with a 25-μl loop.
4. Capillary GC-MS
The stomach contents extract was analysed by capillary GC-MS using a Carlo Erba Fractovap Series 4160 GC (Erba Science, Swindon, Wiltshire) coupled to a VG Micromass 12-12F quadrupole MS (VG Masslab, Altrincham, Cheshire). The GC column was a 12-m bonded phase BP-1 capillary (SGE, Milton Keynes, Buckinghamshire) which led directly into the ion source of the MS. The carrier gas was helium at an inlet pressure of 1.3 kg/cm². The injector temperature was 250°C. Splitless injections (0.5 μl) were made and the injection port was vented after 50 s. The column was held at 100°C for 1 min after injection and was then raised to 280°C at approximately 40°C/min. The MS was operated in the electron impact mode with an accelerating voltage of 70 eV. The interface temperature was 250°C and the source temperature was 200°C. Multiple ion detection was used to monitor LSD ions of m/e 323 (molecular ion) and 181.
Results and discussion
LSD was detected by RIA in all the samples. The levels found are given in Table 1 and may include a response to cross-reacting metabolites in addition to unchanged LSD.
Ante-mortem plasma (Fig. 1) and stomach contents extracts were analysed for LSD by HPLC. A peak with a retention identical to that of authentic LSD was detected in each extract. Comparison of the peak heights with those of known concentrations of LSD gave the levels shown in Table 1.
TABLE 1
LSD LEVELS FOUND BY RIA AND HPLC
| Sample | LSD (ng/ml) found by: | |
|---|---|---|
| RIA | HPLC | |
| Ante-mortem serum | 14.4 | — |
| Ante-mortem plasma | 14.8 | 8 |
| Post-mortem blood | 4.8 | — |
| Stomach contents | 55.2 | 60 |
| Liver blood | 7.2 | — |
Fig. 1. HPLC of ante-mortem plasma extract. Conditions as described in the text; 25 μl injected. The unlabelled peak (solvent front) is typical of that observed with control samples.
The results compared reasonably well with those obtained by RIA. Coextractives or insufficient sample precluded HPLC analysis of the other samples.
The stomach contents extract was analysed by capillary GC-MS. Ions of m/e 323 and 181 were monitored by multiple ion detection and gave peaks with a retention of 10.0 min. Identical results were obtained with authentic LSD. The other samples were not examined by capillary GC-MS.
It is difficult to assess the significance of the results in Table 1 since no fatal levels of LSD in humans are given in the literature. The highest plasma level of LSD previously found [4] was 9.5 ng/ml, and was the mean plasma level of 5 subjects 5 min after intravenous injection of 2 μg LSD/kg. Individual levels were not given. In the same study, the half-life of LSD in plasma was calculated to be 175 min. In another study [5], 13 subjects were each given 160 μg LSD orally and plasma levels of LSD were measured at intervals up to 5 h. The highest level found in any subject was 8.8 ng/ml after 130 min. The other plasma levels in these studies were generally much lower, as were the plasma levels found in other cases of LSD ingestion [3,6,7]. In one previous case in this laboratory (unpublished results), we found LSD in both blood and stomach contents at levels of 7.6 and 11.6 ng/ml, respectively. In a further five cases in which we found LSD in stomach contents, the blood levels were below the RIA detection limit (2.8 ng/ml). In four cases in which LSD was detected in blood, but stomach contents were not available for analysis, the levels ranged from 4.4 to 8.0 ng/ml. The levels found in the ante-mortem samples in the present case (Table 1) are thus nearly double the highest levels previously found in blood.
References
1 R.N. Smith, Immunoassays in forensic toxicology. In J.S. Oliver (ed.), Forensic Toxicology, Croom Helm, London, 1080, pp. 34—47.
2 B. Law, P.A. Mason, A.C. Moffat and L.J. King, A novel ¹²⁵I-radioimmunoassay for the analysis of Δ⁹-tetrahydrocannabinol and its metabolites in human body fluids. J. Anal. Toxicol., 8 (1984) 14—18.
3 W.A. Ratcliffe, S.M. Fletcher, A.C. Moffat, J.G. Ratcliffe, W.A. Harland and T.E. Levitt, Radioimmunoassay of lysergic acid diethylamide (LSD) in serum and urine using antisera of different specificities. Clin. Chem., 23 (1977) 169—174.
4 G.K. Aghajanian and O.H.L. Bing, Persistence of lysergic acid diethylamide in the plasma of human subjects. Clin. Pharmacol. Ther., 5 (1964) 611—614.
5 D.G. Upshall and D.G. Wailling, The determination of LSD in human plasma following oral administration. Clin. Chim. Acta, 36 (1972) 67—73.
6 B. Widdop, The detection of LSD in biological fluids. Bull. Int. Assoc. Forensic Toxicol., 7 (1971) 6—7.
7 P.J. Twitchett, S.M. Fletcher, A.T. Sullivan and A.C. Moffat, Analysis of LSD in human body fluids by high-performance liquid chromatography, fluorescence spectroscopy and radioimmunoassay. J. Chromatog., 150 (1978) 73—84.
Fysh, R. R. 1985. A fatal poisoning with LSD. Oon, M. C., Robinson, K. N., Smith, R. N., White, P. C., Whitehouse, M. J. Forensic Sci Int, 28(2), 109–13 10.1016/0379-0738(85)90067-2
Last edited:

