

lookbehindyou
Greenlighter
- Joined
- Dec 10, 2015
- Messages
- 18
Ihave a little problem. I was a former H user (10 years IV) and contracted HCV after year 5. 2 Years ago i treated with pegylated Interferon-alpha, Sovaldi and Ribavirin for 12 weeks and cleared the virus.
the problem is the following.
Treatment has blasted my brain immune system (consisting of cells called microglia). These cells are now going insane and produce ROS (reactive oxygen species) that attack the nerve tissue and lead to unbelievable memory loss. (i try to explain the magnitude of this memory loss. for example, i take my HiFi from my buddys room onto a table infront of my buddys room door, go to my room and forget what i did actually. ) I forget what my parents names are. I forget my birthday date etc.
) I forget what my parents names are. I forget my birthday date etc.
So, i take curcumin in a high dose to contain the damage the microglia cells are doing to the brain tissue. Curcumin inhibits TLR4, a receptor that is crucial for the activity of microglia. This is unfortunately not the solution. There is still no normal brain functioning and the next step will be this:
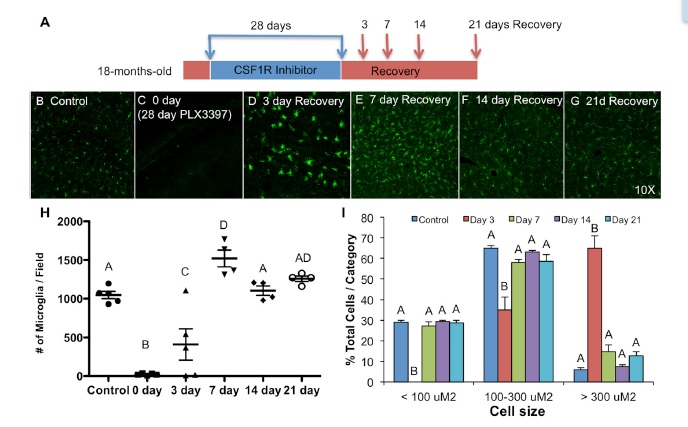
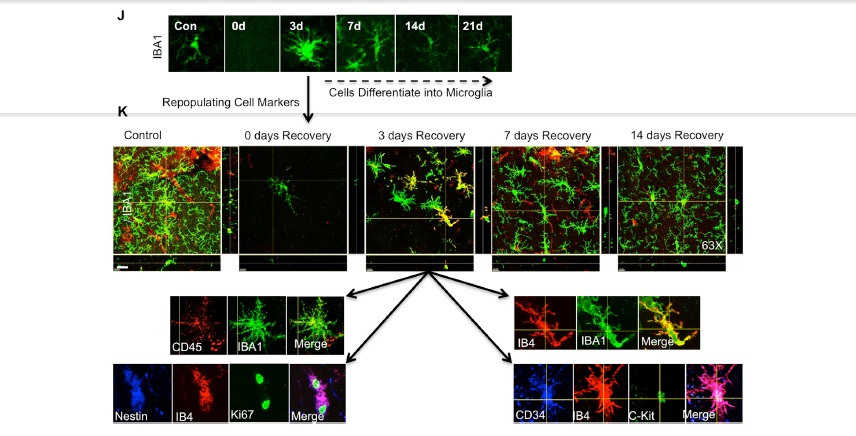
There's a drug in development called PLX3397 (Pexidartinib). This is an anti cancer drug. It inhibits the CSF1R (Colony Stimulating Factor 1 Receptor) that is crucial for the survival of microglia cells. The following link can describe the mode of action:
http://www.alzforum.org/news/research-news/microglial-magic-drug-wipes-them-out-new-set-appears
My question now, can this cure my condition? Is it a good approach?
thanks guys")
the problem is the following.
Treatment has blasted my brain immune system (consisting of cells called microglia). These cells are now going insane and produce ROS (reactive oxygen species) that attack the nerve tissue and lead to unbelievable memory loss. (i try to explain the magnitude of this memory loss. for example, i take my HiFi from my buddys room onto a table infront of my buddys room door, go to my room and forget what i did actually.
) I forget what my parents names are. I forget my birthday date etc.So, i take curcumin in a high dose to contain the damage the microglia cells are doing to the brain tissue. Curcumin inhibits TLR4, a receptor that is crucial for the activity of microglia. This is unfortunately not the solution. There is still no normal brain functioning and the next step will be this:
There's a drug in development called PLX3397 (Pexidartinib). This is an anti cancer drug. It inhibits the CSF1R (Colony Stimulating Factor 1 Receptor) that is crucial for the survival of microglia cells. The following link can describe the mode of action:
http://www.alzforum.org/news/research-news/microglial-magic-drug-wipes-them-out-new-set-appears
My question now, can this cure my condition? Is it a good approach?
thanks guys



 ) I did a MRI 18 months ago unsuspicious. PLX 3397 was designated as breakthrough drug in late october, so i guess it will get approved in late 2016 / 2017. I get the crude substance (HCl salt) from a website for $10.000 / 37.000mg. They fed 290mg/kg PLX3397 to wild type mice for 21 days. That eradicated 99% of their microglia brain-wide. The H.E.D. is therefore 1.600mg/day. A treatment duration of 37 days @1000mg/day equals 37.000mg.
) I did a MRI 18 months ago unsuspicious. PLX 3397 was designated as breakthrough drug in late october, so i guess it will get approved in late 2016 / 2017. I get the crude substance (HCl salt) from a website for $10.000 / 37.000mg. They fed 290mg/kg PLX3397 to wild type mice for 21 days. That eradicated 99% of their microglia brain-wide. The H.E.D. is therefore 1.600mg/day. A treatment duration of 37 days @1000mg/day equals 37.000mg.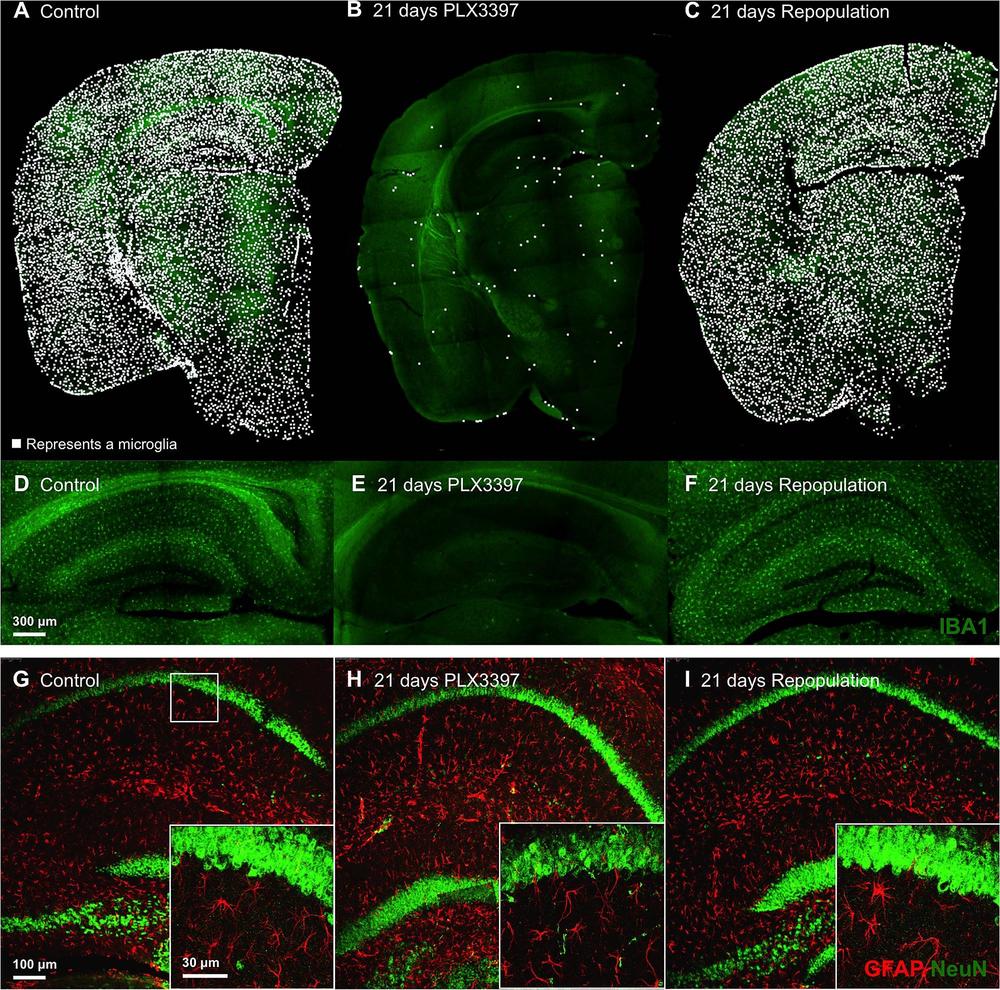

")
