DeathIndustrial88
Bluelighter
- Joined
- Jan 23, 2020
- Messages
- 2,944
So.. Has there been any substantial evidence come out at all yet that norbupe is indeed active in lower dosages of bupe? And if so, can anyone please provide that evidence? Thanks.
Yeah norbupre is thought to have a higher affinity for mu, delta and kappa opioid receptors. Other metabolites could also play a role depending on the dose of buprenorphine administered.So.. Has there been any substantial evidence come out at all yet that norbupe is indeed active in lower dosages of bupe? And if so, can anyone please provide that evidence? Thanks.
Based on what Ive seen, not necessarily metabolize it faster, but the withdrawals 100% will start faster.Also, will long term use of a drug start to make you metabolize that drug at a faster rate once your body is accustomed to it?
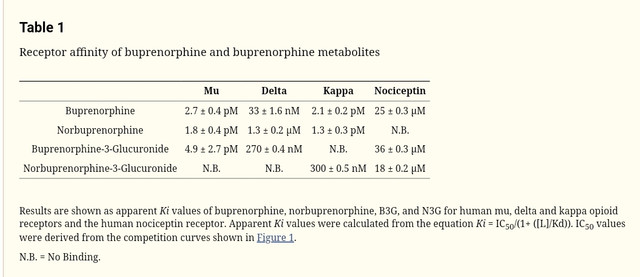
Yeah norbupre is thought to have a higher affinity for mu, delta and kappa opioid receptors. Other metabolites could also play a role depending on the dose of buprenorphine administered.
(Lower number = higher affinity)
Also according to this source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3560935/
"Norbuprenorphine is a potent opioid agonist, with high affinities for mu, delta, and kappa opioid receptors.22
In rats, norbuprenorphine caused dose-dependent respiratory depression and was 10 times more potent than buprenorphine.8,23
Norbuprenorphine respiratory depression was opioid-receptor mediated, and also antagonized by buprenorphine.8 "
Based on what Ive seen, not necessarily metabolize it faster, but the withdrawals 100% will start faster.
") I've noticed this with bupe lately. I use to be able to skip a few days in between doses and be just fine. But now, lately, i've noticed that if I try to do this, I won't necessarily feel full blown withdrawal, but I do feel very "blah" and "off" until I finally take my dose for the day.
I've noticed this with bupe lately. I use to be able to skip a few days in between doses and be just fine. But now, lately, i've noticed that if I try to do this, I won't necessarily feel full blown withdrawal, but I do feel very "blah" and "off" until I finally take my dose for the day. 
Yeah, dont forget its about 50 times stronger than morphine. Its not a good drug but its a really useful "medicine". Basically meant for people who need/want to take something daily but werent so heavy on their past use. I have two friends who both started bupre 5 years ago, one used 30% or something less bupre and he has 200% or more lesser withdrawals. Remember, its closer to fentanyl than morphine. I use 1mg at most per day and its really easy to quit.
Np, I like bupre too.
Well I'm really not sure, once you start looking into it the picture becomes more and more complex haha. I haven't researched it enough.Wow!! Thank you so much for the response, I appreciate it very much!
So theoretically, if one were to take a low enough dose of buprenorphine, the effects felt SHOULD be a combination of norbupe & bupe effects + metabolites? So buprenorphine in low doses would essentially be a pro-drug for a full agonist.
I wonder at what dose buprenorphine would antagonize it's own metabolite then. Thank you for sharing this. I've always wondered why lower doses seemed to feel much better, but I always assumed it had something to with the blood levels spiking up and down from the bupe doses, as I thought norbupe didn't really cross the blood brain barrier.
Well I'm really not sure, once you start looking into it the picture becomes more and more complex haha. I haven't researched it enough.
I believe it's true that norbupe has a hard time crossing the BBB via passive diffusion but, since it has such a high affinity for the opioid receptors, only a very small amount would be needed.
Also there are active transporters which can get opioids in and out of the brain, I think this has been shown for morphine and its active metabolite M-6-G, a protein actuallyhelps them cross the BBB.
I read that norbupe, but apparently not bupe itself, is actually actively excreted out of the brain by P-glycoprotein transporters. Maybe it can also get into the brain with the help of another transporter?
Additionally, while most p450 enzymes are found in the liver, some of them have also been found within the brain so it's possible that bupe could also be metabolized there to some extent, and since it's so potent even a small amount could have an impact in its effects.
I just now saw your location. LOL, great one.
I would use more than 1mg a day, but I cant afford that shit since I use it illegally. And bupre works different the each time, well atleast almost. Stopping daily use since the fun is gone at this point.
Yeah there's the old saying "less is more" with bupe, but of course it also depends on your previous opioid use. Seems bupe has a ceiling where high doses stop acting like a pleasurable opioid and only keep WD away and block other opioids, I've heard it stops being "recreational" after 1-2mg.Interesting. Thank you for your valuable insight.
I guess it's technically still up in the air as to whether norbupe truly elicits an effect or not. Like schizopath said, bupe seems to feel different every time and at varying doses. I would love to be able to find a dose that keeps the opiate-effect and euphoric effect consistent, but have been unable (even after 5 years) to determine what dose this might be. Seems like it's too complex of a drug to really know for sure.
But I do believe the higher doses are almost pointless. Countless times I have actually become very dysphoric after using anywhere from 8-12mg of buprenorphine.
I asked this question as I am on bupe for maintenace, but it is no longer helping with cravings as I don't feel jack shit from it and this is unfortunate because it's effecting me mentally and making me crave heroin again daily. And methadone is not an option for me at the moment, so I'm trying to figure out the best way to utilize what I have and actually feel like my mind is satisfied. I have, in the past achieved very beautiful effects from bupe, so I know it's possible to feel good with this medication. but then again I also had a lower tolerance.
I truly appreciate everyone's input and responses. If anyone else has anything else to add, please feel free.

 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
Put aside the Norbupe thing for a minute. If you have a 2mg dose and take 2mg 24hrs later, you're accumulating the drug. At that rate you never really have time coming down from the high so you'll never really be high. Lower doses seem to prevent that buildup.
Thru trial and error I found my bupe ceiling was around 2mg. More would do nothing. So I decided to stick to .5-1mg a day and if I really needed a buzz I could bump it up to 1-2mg and truly get twice the effect.
Tapering to 2mg was no problem at all for me, going to 1mg was a little weird but nothing that bad.
I don't think so because the primary role of P-gp is to get molecules/drugs out of the cell. I guess in this case they're talking about breast cells (maybe cancer cells in general) but P-gp is expressed in almost every cell and it can also get drugs OUT of the blood brain barrier as far as I know. So a P-gp inhibitor would essentially prevent certain drugs from being thrown out (which is kinda like a natural defence mechanism of the cell), thus increasing their intracellular concentration which often means a stronger effect.Maybe some one who understands what is said here better can chime in, but from what I understand, norbuprenorphine & buprenorphine inhibit P-gp, so that should allow norbupe to cross the blood brain barrier right? Wouldn't this also allow drugs like loperamide to cross the blood brain barrier?
Of course this info was taken from something about breast cancer, so maybe I'm misunderstanding something.
Interaction of drugs of abuse and maintenance treatments with human P-glycoprotein (ABCB1) and breast cancer resistance protein (ABCG2) - PubMed
Drug interaction with P-glycoprotein (P-gp) and breast cancer resistance protein (BCRP) may influence its tissue disposition including blood-brain barrier transport and result in potent drug-drug interactions. The limited data obtained using in-vitro models indicate that methadone...
I don't think so because the primary role of P-gp is to get molecules/drugs out of the cell. I guess in this case they're talking about breast cells (maybe cancer cells in general) but P-gp is expressed in almost every cell and it can also get drugs OUT of the blood brain barrier as far as I know. So a P-gp inhibitor would essentially prevent certain drugs from being thrown out (which is kinda like a natural defence mechanism of the cell), thus increasing their intracellular concentration which often means a stronger effect.
At least that's the case with some anticancer drugs, P-gp is often overactive in cancer cells so the drugs don't work as well because the fucked up cell is constantly getting rid of them. Inhibiting P-gp makes those drugs more efficient.