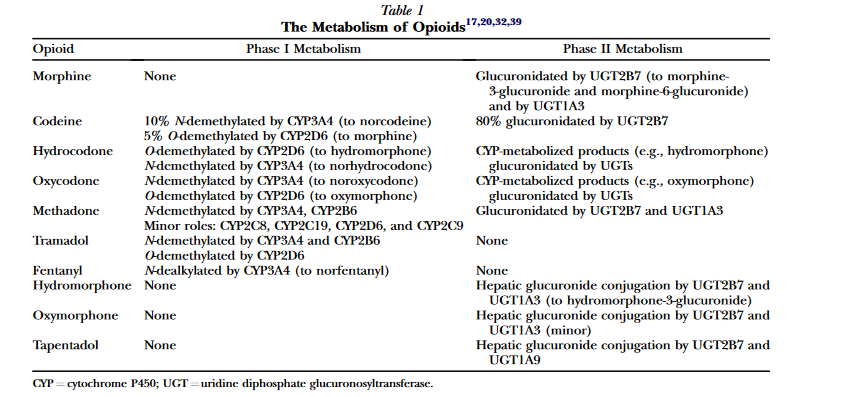
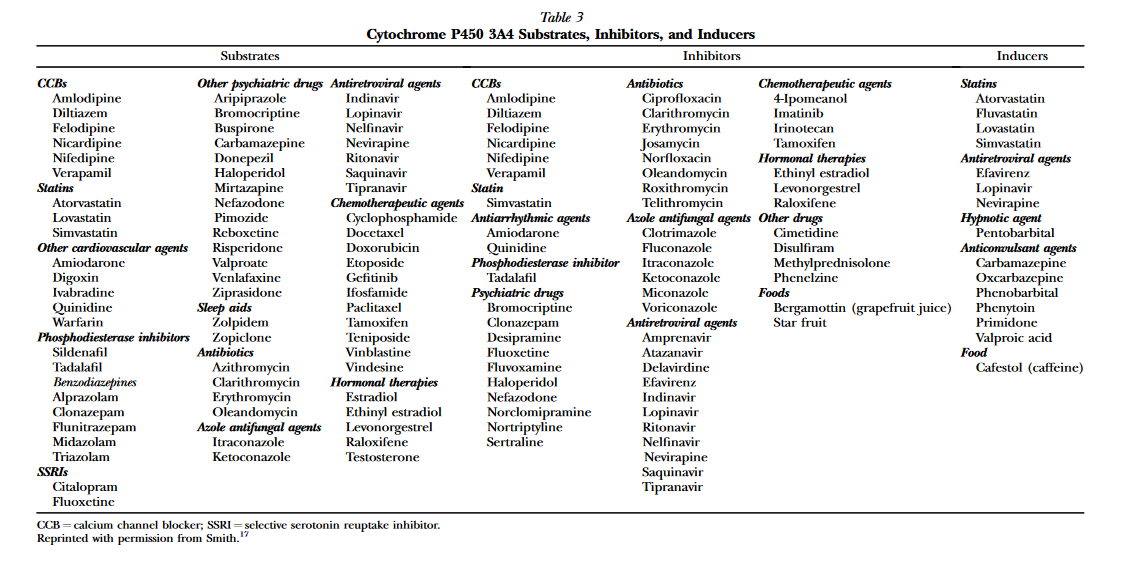
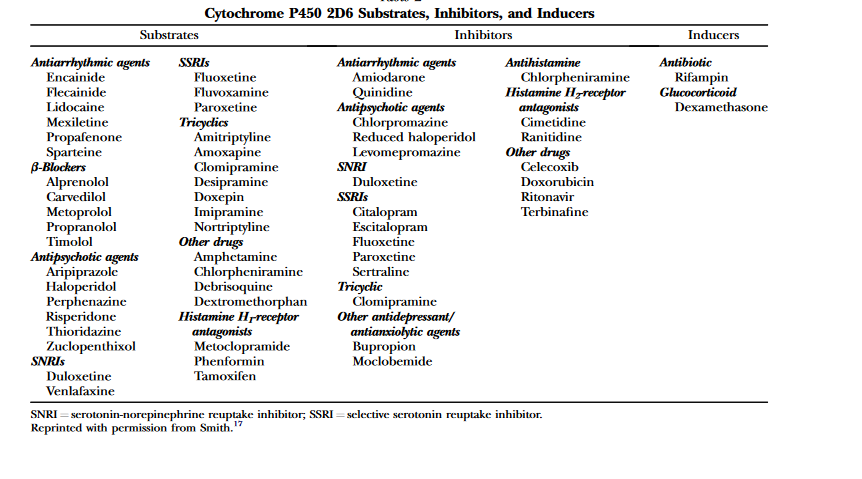
As the title says, is morphine/opium affected by SSRIs/SNRIs? What about antidepressants that affect dopamine like NDRIs? I have read studies that say that some effects of morphine are actually increased by these medications, but it only mentioned medical purposes and not euphoria or anything like that. But I am wondering if it might actually hinder the recreational value, by reducing euphoria. I have tried to use morphine/opium while on an SARI called Trazodone and that completely negated the euphoria, but Trazodone works differently and affects the receptors that are responsible for releasing dopamine. I know that these medications do work on the same enzyme as codeine does to turn into morphine and would probably screw that process up, but as far as I know, SSRIs/SNRIs shouldn't really affect morphine/opium as it does not need to do that and go through that enzyme. I am unsure about NDRIs and stuff like that. Thanks.
Last edited: