^ Pretty much all the dissociatives out other than Ketamine are SRIs (Serotonin Reuptake Inhibitors) and that's usually what produces the "opiate like euphoria" that some of them have.
Some examples:
- 3-MeO-PCP
- 4-MeO-PCP
- Methoxetamine (MXE)
- DXM
Some are also dopamine reuptake inhibitors, like PCP, and likely 3-MeO-PCP too.
Stimulant dissociatives are not a new thing, the only non-stimulant dissociatives I can think of off the top of my head are Nitrous Oxide and Ketamine
")
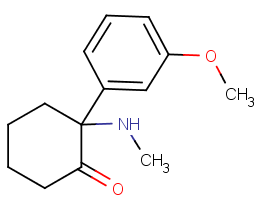
Also none of those have any opioid activity, aside from DXM (although DXO, DXM's main metabolite doesn't really have any), despite how many times people have made comments about MXE and 3-MeO-PCP feeling "opiate like". There's no reason this would be any different, since structurally it's smack bang in the middle between Ketamine and Methoxetamine.
If anything I'd say rather than certain dissociatives being opiate like, it's more like low doses of dissociatives are anti-depressant like. Anti-depressants also generally being SRIs, like most dissociatives. Opiates have a similar anti-depressant quality to them, though it's not due to serotonergic activity, feels a tad different, and is easy enough to tell apart once you've been using opiates for years on end in my experience.
The fact your girlfriend got little adds even more to the likelihood that this is an SRI like MXE etc, since you mentioned she had abused MDMA, and MDMA abuse leads to down-regulation of the serotonin transporters, along with serotonergic neurotoxicity and lasting damage.



")

