fastandbulbous said:
^ The degree of analgesia is in a round about way linked to the euphoria as opiates don't effectively block pain, but prevent the emotional response to pain (fear being the main one). the fear of pain being by far the biggest contributor to pain's distressing effects
This is only partially true. Pain transmission via the ventral funiculus (spinothalamic tract for pain/temperature info, where they used to perform tractotomy to stop horrid pain) is also inhibited by opioids directly.
Euphoria, emotional response to pain, and nociception sent by fast (A-class, fat and myelinated) neurons in the spinothalamic tract are ALL altered by opiates through mu-opioid agonism, BUT they key here is that functional specialization/regionalization in the brain complicate things. The ability to cross ependymal BBB cells as measured by the octanol:water coefficient (and brain uptake index, which no-one here ever mentions) is only the surface on wackyness. Epithelial cells are not all the same, and some evidence says different drugs may cross differentially depending on what arteries feed different gross brain areas, look up leaky epithelial cells). The nuclei (neuroanatomical nucleus, not a cellular nucleus) end up having different threshold concentrations and dose-response curves because of excitatory and inhibitory modulation for different ligands. Etc, etc, etc.
--------------------------------------------------
I'll stop blabbering on but, if you are interested and want to go on a wikipedia-fest:
-Euphoria is mediated by the VTA for opioids (also complicated by the GABA "switch", where opioids seem to stop needing to act on the GABA inhibitory neurons, and work directly on the DA after entrainment)
-"Emotional" responses to pain by the PAG (periaqueductal grey, ventrolateral area which can be stimulated electircally to produce a nod-like posture AKA quiescence)
-Actual pain transmission via the spinothalamic tract in the ventral funiculus.
------------------------------------------------------
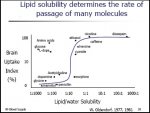
Also, I'm going to be an information pirate and share an image that I'm sure a lot of you will enjoy which will kind of highlight your idea F&B (although I did just semi-refute it). It graphs octanol:water coefficient vs brain uptake index. This was the first study to do this, so the data was ancient but mini-revolutionary.
-You can compare heroin and morphine on there to see that even though heroin and morphine have a similar octanol:water coeff., they are taken up by brain tissue very differently.
-It shows why diazepam gets sucked up by fat tissue, and therefore has a cumulating effect.
-And it shows also how saying things like DA "doesn't cross the BBB" is a little simplified.
-Also, it shows how L-dopa uses transporters to completely not fit the trend.




") tnx 4oh putting up w/ the rant.
tnx 4oh putting up w/ the rant.