ebola?
Bluelight Crew
Deprenyl is a rather fine substitute to most of the traditional stimulant medications currently employed in the states.
Well, l-deprenyl is pretty commonly prescribed, even off-label (eg, for depression).
ebola



N&PD Moderators: Skorpio
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
Ketamine salts solubility
![]()
ebola?
Bluelight Crew
Deprenyl is a rather fine substitute to most of the traditional stimulant medications currently employed in the states.
Well, l-deprenyl is pretty commonly prescribed, even off-label (eg, for depression).
ebola
![]() I have theories of my own, but can someone explain why/how the anti-depressant/mood elevating effect of stimulants disappears over chronic use (assuming it does) whilst that of MAOIs doesn't?
I have theories of my own, but can someone explain why/how the anti-depressant/mood elevating effect of stimulants disappears over chronic use (assuming it does) whilst that of MAOIs doesn't?
![]()
Epsilon Alpha
Bluelighter
http://www.rifters.com/real/Blindsight.htm
Probably the best work of fiction I've read over the last five years, with a close second coming to the lesswrong.com cofounder.
And @Ho-Chi-Minh, I believe its partially due to the differential regulation of the NA/DA vs 5HT systems though I am not in the state to argue either way currently (woot! Odd sleep disorders!)
![]()
SONN
Bluelighter
Can anyone give me a reason why this drug wouldn't be fun?
http://isomerdesign.com/PiHKAL/explore.php?domain=pk&id=306
maybe add an N-methyl?
I'd like to know more about why the 4-chloro position might be better/worse for you than, for instance, a 4-methyl or 4-methoxy? I mean in effects and toxicity.
perhaps i'm just missing out a lot because I don't have the physical version of pihkal but I feel like there could be a really basic phenethylamine substitution that is being massively overlooked. Maybe it wouldn't get you extremely fuckedddd upppp or whatever but more of just a basic stimulant/empathogen that can provide relatively harmless 5-ht release or something useful like that.
is there a resource where Nichols has data on https://en.wikipedia.org/wiki/6-CAT and possibly more of his non-neurotoxic compounds?
bloodshed344
Bluelighter
Can anyone give me a reason why this drug wouldn't be fun?
http://isomerdesign.com/PiHKAL/explore.php?domain=pk&id=306
maybe add an N-methyl?
I'd like to know more about why the 4-chloro position might be better/worse for you than, for instance, a 4-methyl or 4-methoxy? I mean in effects and toxicity.
perhaps i'm just missing out a lot because I don't have the physical version of pihkal but I feel like there could be a really basic phenethylamine substitution that is being massively overlooked. Maybe it wouldn't get you extremely fuckedddd upppp or whatever but more of just a basic stimulant/empathogen that can provide relatively harmless 5-ht release or something useful like that.
is there a resource where Nichols has data on https://en.wikipedia.org/wiki/6-CAT and possibly more of his non-neurotoxic compounds?
Put an alpha methyl on the first one for brain damage ")
I don't think an n-methyl will help, try putting the chloro at the 3?
The second one... very interesting.
![]()
pharmakos
Bluelighter
perhaps i'm just missing out a lot because I don't have the physical version of pihkal
there's a LOT of stuff on isomerdesign that isn't in pihkal (including the compound in that link)
![]()
SONN
Bluelighter
^ I meant more of discussion on the meaning and characteristics of the basic phenethylamine chemical structures and how adding parts on changes things and why, Rather than more novel structures.
![]()
babylonboy
Bluelighter
I don't think there's much discussion of SAR in the first part of PiHKAL, the "Extensions and Commentary" sections tend to be the juiciest, the first half is an autobiography, and IMO isn't particularly important.
![]()
pharmakos
Bluelighter
I don't think there's much discussion of SAR in the first part of PiHKAL, the "Extensions and Commentary" sections tend to be the juiciest, the first half is an autobiography, and IMO isn't particularly important.
true, most of the chemistry is in Book 2 and is available on Erowid http://www.erowid.org/library/books_online/pihkal/pihkal.shtml
Book 1 does have some chemistry though, and more background on the order Shulgin did everything in
![]()
sekio
Bluelight Crew
L-Methylphenidate Is Stereoselectively Hydrolyzed by Human Carboxylesterase CES1A1
Zejin Sun, Daryl J. Murry, Sonal P. Sanghani, Wilhelmina I. Davis, Natalia Y. Kedishvili, Qin Zou, Thomas D. Hurley and William F. Bosron
http://jpet.aspetjournals.org/content/310/2/469.long
Clinically relevant doses of methylphenidate significantly occupy norepinephrine transporters in humans in vivo.
Hannestad J, Gallezot JD, Planeta-Wilson B, Lin SF, Williams WA, van Dyck CH, Malison RT, Carson RE, Ding YS.
http://www.ncbi.nlm.nih.gov/pubmed/20691429
Medical Marijuana: Clearing Away the Smoke
Igor Grant, J. Hampton Atkinson, Ben Gouaux, and Barth Wilsey
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3358713
As with all medications, benefits and risks need to be weighed in recommending cannabis to patients. We present an algorithm that may be useful to physicians in determining whether cannabis might be recommended as a treatment in jurisdictions where such use is permitted.
Cannabis is suggested as a treatment option for neuropathic pain, where standard Rx treatments fail, and the risk of substance abuse and mood disorders is judged to be acceptably low. I like that patient preference for oral versus smoked versus vapourised marijuana is part of the treatment too.
Concerns have long been voiced that rapid tolerance to adverse effects might portend tolerance to beneficial effects. Data from studies using oral sprays of cannabinoids or dronabinol in multiple sclerosis report that individuals can reduce the incidence and severity of adverse effects by downward self-titration without loss of analgesia. Other studies in this population note that overall the incidence and severity of adverse effects diminishes over time without evidence of tolerance to analgesic effects. Yet it is rare that clinical trials of cannabinoids extend follow-up beyond 12 weeks, leaving questions on maintenance of gains or need for dose escalation unanswered. One study with 12-month follow-up concluded there may be sustained analgesia for pain associated with multiple sclerosis, where about 30% of cannabinoid-treated participants report continued “improvement” at 12 months compared to about 15% on placebo on doses conservatively limited to a maximum of 25mg THC daily. This suggests that pain relief may be sustained without dose increases. But the study design was not intended to determine the proportion of patients who experienced diminution of effect, or whether dose escalation, even within the set boundary, was needed for maintenance of efficacy.
This is pretty suprising. I don't think one can say the same about the other "habit forming" drugs, esp. opioids and benzodiazepines.
Also:
Sick burn, guys.
The classification of marijuana as a Schedule I drug as well as the continuing controversy as to whether or not cannabis is of medical value are obstacles to medical progress in this area. Based on evidence currently available the Schedule I classification is not tenable; it is not accurate that cannabis has no medical value, or that information on safety is lacking. It is true cannabis has some abuse potential, but its profile more closely resembles drugs in Schedule III (where codeine and dronabinol are listed). The continuing conflict between scientific evidence and political ideology will hopefully be reconciled in a judicious manner [...]
Last edited:
Hi all I wanted to introduce myself and from my reading it state this was the place to do that, I hope. I have been trying for the last 4 months or so to gain knowledge about synths and chemical make up of certain Rx's. Before attempting to do any kind of synths I believe one should have the proper knowledge and background safety of what one will be doing. I'm sorry if this is not the place for this and would like if anyone can point me to the best spot for the knowledge I'm looking for.
![]()
babylonboy
Bluelighter
Yeah sorry mate we don't discuss synthesis here, the Organic Chemistry Lab Survival Manual is a great reference, and there are repositories of information and forums dedicated to drug synthesis, but this is not one of them.
endotropic
Bluelight Crew
Spatiotemporal Brain Dynamics of Emotional Face Processing Modulations Induced by the Serotonin 1A/2A Receptor Agonist Psilocybin.
Abstract
Emotional face processing is critically modulated by the serotonergic system. For instance, emotional face processing is impaired by acute psilocybin administration, a serotonin (5-HT) 1A and 2A receptor agonist. However, the spatiotemporal brain mechanisms underlying these modulations are poorly understood. Here, we investigated the spatiotemporal brain dynamics underlying psilocybin-induced modulations during emotional face processing. Electrical neuroimaging analyses were applied to visual evoked potentials in response to emotional faces, following psilocybin and placebo administration. Our results indicate a first time period of strength (i.e., Global Field Power) modulation over the 168-189 ms poststimulus interval, induced by psilocybin. A second time period of strength modulation was identified over the 211-242 ms poststimulus interval. Source estimations over these 2 time periods further revealed decreased activity in response to both neutral and fearful faces within limbic areas, including amygdala and parahippocampal gyrus, and the right temporal cortex over the 168-189 ms interval, and reduced activity in response to happy faces within limbic and right temporo-occipital brain areas over the 211-242 ms interval. Our results indicate a selective and temporally dissociable effect of psilocybin on the neuronal correlates of emotional face processing, consistent with a modulation of the top-down control.
Nice to see human psychedelic research chugging along, even if the conclusions you can draw from an EEG study are less than stellar. I found this really interesting as well:
Participants were excluded, if they had history of drug dependence, as assessed by a self-made consumption questionnaire, or if they were currently using drugs as assessed by a urine drug test. Nevertheless, seven participants were occasional smokers (<6 cigarettes/day), 7 participants reported a sporadic or rare cannabis use in the past (<2 joints/month), one participant reported previous experience with MDMA (one pill lifetime), and one reported previous experience with psilocybin (one administration lifetime).
All but one of the subjects were totally psychedelic naive! And yet no significant increase in anxiety scores.
Last edited:
I'm trying to track down a certain article, it's not really the purpose of this thread to ask questions like this but I figured someone here could help. Sorry if this is inappropriate.
In this thread (http://www.bluelight.ru/vb/threads/427070-Bupe-SHOULD-block-the-effects-of-Pot-but-doesnt-why): it is said:
researchers have even found it possible to largely recreate the effects of opioid agonists using nothing more than serotonin modulation systems (closed loop) on mU knockout mice.
Does anyone know what is this experiment - a link to the article?
Thanks!
E: Oh and feel free to give me better ideas regarding how to track down the article/experiment in question, I don't think this is very effective 
![]()
sekio
Bluelight Crew
Repeated S-ketamine Infusions in Therapy Resistant Depression: A Case Series
J. Clin. Pharmacol., Sept. 2013 http://onlinelibrary.wiley.com/doi/10.1002/jcph.122/abstract
All six of the evaluated unipolar patients (demographic and clinical characteristics see Table 1) suffered from a major depressive episode according to DSM IV criteriaand had proven to be pharmacoresistant despite stepwise treatment with at least two antidepressants from different biochemical classes given in sufficient dosages for an appropriate duration. No psychiatric and no significant somatic comorbidity could be evaluated. In two patients ECT had been performed before treatment with ketamine infusions. In the other four patients, ECT had been also discussed as a treatment option but was refused by the patients. All patients were informed about the off label therapeutic use and possible side effects of ketamine infusions and gave their written informed consent before initiation of ketamine therapy. Treatment was started with a 40 minute administration of 0.25 mg S ketamine/kg body weight i.v. in the presenceof the psychiatrist and an anesthesiologist. [...] Three patients showed an improvement in depressive symptoms in both the short and the longer term in two patients (one male, one female), the HAMD score indicated remission (see Figure 1 and Table1); in one male patient treatment was discontinued
because a severe dissociative condition was reported after the first administration. One of the female patients also reported pronounced dissociative symptoms.
5/6 is pretty good, I think.
endotropic
Bluelight Crew
Repeated S-ketamine Infusions in Therapy Resistant Depression: A Case Series
J. Clin. Pharmacol., Sept. 2013 http://onlinelibrary.wiley.com/doi/10.1002/jcph.122/abstract
5/6 is pretty good, I think.
On first glance, this looked less promising than I had hoped. A typical result for an SSRI trial is 1/3 no response, 1/3 partial response, 1/3 total remission, and these results match that pattern pretty closely.
On the other hand, the fact that these 6 were all refractory to standard treatment gives enough reason to move ahead to larger trials, I think.
![]()
Incunabula
Bluelighter
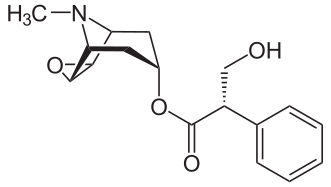
Bloody hell! Scopolamine and cocaine are just this ... close to each other in structure
 and the effects are so different! ha
and the effects are so different! ha
![]()
pharmakos
Bluelighter
that is pretty crazy
cocaine:
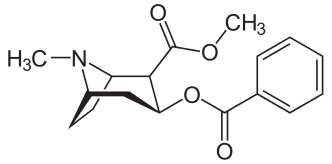
scoploamine:
![]()
ebola?
Bluelight Crew
the study said:
40 minute administration of 0.25 mg S ketamine/kg body weight i.v.
Okay...so for a person of average weight, this is like 17.5 mg pushed over 40 minutes, presumably of the more active enantiomer. I would expect pretty moderate effects. What does this suggest about dosing regimens people should take at home for personal, 'clandestine' treatment of depression?
the study said:
in one male patient treatment was discontinued because a severe dissociative condition was reported after the first administration. One of the female patients also reported pronounced dissociative symptoms.
Okay...so getting high as hell on site is enough to warrant discontinuation of treatment? That doesn't seem fair.
ebola