I very like doing cocaine IV in pretty moderate doses. But this drug is always frustrates me every time due to short time of action and extreme hypertension that comes after the main "dopamine" effect fade out. Basically I very liked mephedropne IV before, that worked like magic and almost not having any problems, while with coke I got uncomfortable hypertension after the main effect. I duuno why but looks like mephedrone has it's own hypotension properties that makes the experience very smooth, or maybe it's because of the serotonin, which cocaine lacks.
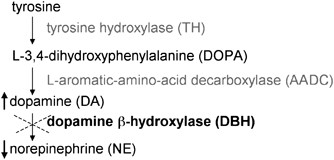
While I study some info I think this happens because large portion of dopamine being converted down to norepinerphine and gets you unpleasant hypertension for about 1-2 hrs after until this gets cleaned. I've already tried to combine coke with lyrica which definately helps but not much. Also I've seen people using low doses of A-blockers like clonidine, but never tied yet. Actually this only deals with the native epinephrine release, but I belive cannot deal with those have been created from the dopamine breakdown.
So, I go and search for the enzyme that doing this and looks like it's -Dopamine β-hydroxylase. So I was thinking what if using a bit of the inhibitor like Fusaric acid or Disulfiram is a potent dopamine β-hydroxylase inhibitor. I'm thinking if this working it's also can potentiate and prolongate the cocaine high while blocking the unwanted effects. Does anyone tried it ? Is it safe to use?
While I study some info I think this happens because large portion of dopamine being converted down to norepinerphine and gets you unpleasant hypertension for about 1-2 hrs after until this gets cleaned. I've already tried to combine coke with lyrica which definately helps but not much. Also I've seen people using low doses of A-blockers like clonidine, but never tied yet. Actually this only deals with the native epinephrine release, but I belive cannot deal with those have been created from the dopamine breakdown.
So, I go and search for the enzyme that doing this and looks like it's -Dopamine β-hydroxylase. So I was thinking what if using a bit of the inhibitor like Fusaric acid or Disulfiram is a potent dopamine β-hydroxylase inhibitor. I'm thinking if this working it's also can potentiate and prolongate the cocaine high while blocking the unwanted effects. Does anyone tried it ? Is it safe to use?
Last edited: