Hey, I’ve had tension headaches, chronic fatigue and brain fog for 12 years. Before that I took mcat and mdma on weekends for about 3 years. I eat well, sleep well, exercise and minimise stress. I’ve basically completed the NHS and im no better. Brain fog is the worst! I feel like an idiot 24/7.
I did develop ibs at the same time so I have noticed a link between poor gut health and brain fog. Have you had any gut issues?
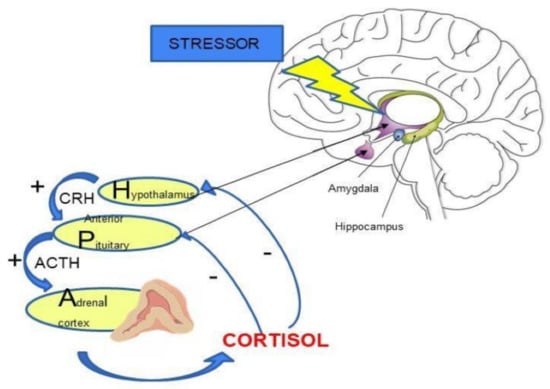
The chronically elevated cortisol, norepinephrine and other stress hormones due to the constant fight or flight caused by the HPA axis disregulation leads to depletion of both magnesium and potassium.
Stress hormones and deficiency and potassium in magnesium as well as depletion of B vitamins due to stress hormones will give you brain fog.
You have to fix the HPA axis dysregulation.
Large doses of B complex vitamins. Doses of 500 mg a day of thiamine, 100mg a day of B6, 1000 mcg a day of B12 are needed to start.
I think your IBS is due to the stress from the HPA axis dysregulation.
Enhanced stress responsiveness has been implicated as a potential mechanism contributing to the pathophysiology of irritable bowel syndrome (IBS), and should be reflected in altered function of the hypothalamic-pituitary-adrenal (HPA) axis and the sympathetic ...
Everything I've read says the hospital could do a blood test and it's not a big deal.
That said, I don't necessarily think magnesium deficiency is the cause. I believe it is a symptom.
Chronically elevated cortisol, adrenaline/ norepinephrine, and other hormones drastically deplete the body of magnesium. Magnesium. When the body is depleted of magnesium, it leaks potassium from the kidneys.
The proximal cause is HPA axis dysregulation, downstream effects include hormonal issues as well as magnesium and potassium deficiency.
Like I said a blood test won’t detect magnesium deficiency unless you’re really really low because your body tightly regulates it. Which is why it goes under the radar. I believe you have to test the cells which is really expensive to do.
Im not really sure what HPA axis dysregulation is. I’m not saying you’re wrong. What i am saying is, I have helped people with a simple dose of magnesium come out of LTC. I have talk to G_chem, who was the user that I first learned this from, and he has told me he has helped numerous people. I’ve seen it transform my friend who was in living hell, bring life back into her eyes.
Why not just try it and see if it works? It’s a low risk/high reward decision. I’ve seen magnesium get dismissed over and over on this forum. What if it was really that simple like what Autotripper said?
Like I said a blood test won’t detect magnesium deficiency unless you’re really really low because your body tightly regulates it. Which is why it goes under the radar. I believe you have to test the cells which is really expensive to do.
Im not really sure what HPA axis dysregulation is. I’m not saying you’re wrong. What i am saying is, I have helped people with a simple dose of magnesium come out of LTC. I have talk to G_chem, who was the user that I first learned this from, and he has told me he has helped numerous people. I’ve seen it transform my friend who was in living hell, bring life back into her eyes.
Why not just try it and see if it works? It’s a low risk/high reward decision. I’ve seen magnesium get dismissed over and over on this forum. What if it was really that simple like what Autotripper said?
First of all, there is a test, a simple blood test. If you're below 1.7, that means you're deficient. If you below 1.4 that means you're severely deficient.
I have literally had that blood test done on me. Probably 10 times because for years I abused alcohol and that leads to magnesium deficiency. Most of the time I was normal, a couple times I was low.
So they absolutely can test for it and find a deficiency.
A serum magnesium test measures the level of magnesium in the blood. Alternative Names: Magnesium - blood. How the Test is Performed A blood sample is needed.
I understand that there are blood test for it. i don’t think you understand that the body tightly regulates magnesium. if you’re low, your body will take magnesium from other places in your body like your bones to try to keep it in the normal range because it’s so important. A serum test won’t always detect that your body is low and taking magnesium from other places to compensate. The mag levels in a serum test could just look like it’s normal.
Look, I don’t really care if I’m right or wrong. I just want to share my story and to see if it will help other people. Dont get so caught up in trying to be right and think everyone else is wrong. Your intentions aren’t in the right place. This isn’t about you or me. It’s about helping people.
Hey, I’ve had tension headaches, chronic fatigue and brain fog for 12 years. Before that I took mcat and mdma on weekends for about 3 years. I eat well, sleep well, exercise and minimise stress. I’ve basically completed the NHS and im no better. Brain fog is the worst! I feel like an idiot 24/7.
I did develop ibs at the same time so I have noticed a link between poor gut health and brain fog. Have you had any gut issues?
First of all, there is a test, a simple blood test. If you're below 1.7, that means you're deficient. If you below 1.4 that means you're severely deficient.
I have literally had that blood test done on me. Probably 10 times because for years I abused alcohol and that leads to magnesium deficiency. Most of the time I was normal, a couple times I was low.
So they absolutely can test for it and find a deficiency.
A serum magnesium test measures the level of magnesium in the blood. Alternative Names: Magnesium - blood. How the Test is Performed A blood sample is needed.
Magnesium is a critical mineral in the human body and is involved in ~80% of known metabolic functions. It is currently estimated that 60% of adults do not achieve the average dietary intake (ADI) and 45% of Americans are magnesium deficient, a ...
www.ncbi.nlm.nih.gov
“Once magnesium is absorbed it is distributed throughout the body for use and storage. Only 0.8% of magnesium is found in blood with 0.3% in serum and 0.5% in erythrocytes, with a typical total magnesium serum concentration between 0.65–1.0 mmol/L [89,90]. The rest is distributed in soft tissue (19%), muscle (27%), and bone (53%) (Figure 6) [89,90,91]. Up to one-third of the magnesium stored in bone is exchangeable [92], and while the total amount of magnesium stored in bone can change with age, bone remains the most significant area of stored and exchangeable magnesium.”
First of all, there is a test, a simple blood test. If you're below 1.7, that means you're deficient. If you below 1.4 that means you're severely deficient.
I have literally had that blood test done on me. Probably 10 times because for years I abused alcohol and that leads to magnesium deficiency. Most of the time I was normal, a couple times I was low.
So they absolutely can test for it and find a deficiency.
A serum magnesium test measures the level of magnesium in the blood. Alternative Names: Magnesium - blood. How the Test is Performed A blood sample is needed.
“Understanding the relationship between the concentration of an analyte in the compartment being measured (e.g., blood, urine, and epithelial samples) and the status of that analyte in the body, or its relevance in the measured compartment is a fundamental principal that will render an analytical test useful or not. Due to the way in which magnesium is compartmentalized, the typical compartment (blood and urine) analytics may not provide an accurate proxy of magnesium status and will mislead the practitioner.”
3.1 blood levels
“The current “normal” range interval of serum magnesium is 0.7–1 mmol/L and was established based on serum magnesium levels gathered by a U.S. study between 1971 and 1974 of presumably healthy individuals aged 1–74 years [120]. Serum changes can be influenced by dietary magnesium intake and albumin levels, but can also be affected by short term changes like day to day and hour to hour variability of the amount of magnesium absorbed and excreted through the kidneys [121]. Blood levels have been shown to increase in response to magnesium supplementation, but this does not signal that complete equilibrium has been established between blood and the nearly 100-fold larger body reservoir of magnesium. In fact, the much larger exchangeable pool of magnesium is more often called upon to augment blood levels to maintain a narrow range preferentially, which is a key reason why blood measurements can easily mask deficiency [122,123].
The tight control of magnesium serum levels, representing only 0.8% of total body stores (see Section 2.4), therefore serves as a poor proxy for the 99.2% of magnesium in other tissues that constitutes the body’s true magnesium status. Furthermore, this narrow serum range feeds the common perception of clinicians that magnesium levels rarely fluctuate, and therefore, are not indicative of the condition for which the blood tests are ordered. Therefore, practitioners are apt to order blood tests for magnesium infrequently, if at all, and if a magnesium level is in the patient chart, it is more often as part of a blood test panel and not purposely ordered to determine the magnesium status [89,124,125,126]. This contributes significantly to magnesium deficiency not being recognized as a modifiable nutritional intervention, and magnesium in general, being the neglected mineral that it is.
Red blood cells’ (RBC; erythrocyte and monocyte) magnesium levels are often cited as preferable to serum or plasma levels due to their higher magnesium content (0.5% vs. 0.3%, respectively). Some RBC studies report correlation to magnesium status particularly when subjects are placed on long-term (~3 months) magnesium replete or deplete diets. However, most studies using RBC magnesium endpoints do not satisfy this long-term design and have not been performed in nearly enough randomized clinical studies to be considered sufficiently robust or reliable (Table 1) [127,128,129]. In addition, the majority of RBC studies do not validate the method through inter-compartmental sampling (e.g., urine and muscle), challenging the claim that this test is a reliable representation of the large magnesium pool.”
Magnesium is a critical mineral in the human body and is involved in ~80% of known metabolic functions. It is currently estimated that 60% of adults do not achieve the average dietary intake (ADI) and 45% of Americans are magnesium deficient, a ...
So I had an LTC years ago and can confirm the HPA axis theory. I had many tests done and my pregnenolone, testosterone levels were low and my saliva cortisol was blunted. Doing HCG+TRT+Preg supplementation and time worked for me and alleviated my anxiety.
I think the key is whether one has anhedonia though. HPA axis dysfunction alone will cause anxiety and low mood but not anhedonia in my experience. Anhedonia is typically going to be more than just a dysfunction of the HPA axis, like perhaps an alteration in allopregnanolone levels as well. I think the medication Zuranolone on the horizon could very well be an LTC cure.
As far as magnesium, the serum tests aren't that accurate. RBC Magnesium blood test is what you want to get to check the cellular level of Mg. There's more written about this in the book The Magnesium Miracle.
“Understanding the relationship between the concentration of an analyte in the compartment being measured (e.g., blood, urine, and epithelial samples) and the status of that analyte in the body, or its relevance in the measured compartment is a fundamental principal that will render an analytical test useful or not. Due to the way in which magnesium is compartmentalized, the typical compartment (blood and urine) analytics may not provide an accurate proxy of magnesium status and will mislead the practitioner.”
3.1 blood levels
“The current “normal” range interval of serum magnesium is 0.7–1 mmol/L and was established based on serum magnesium levels gathered by a U.S. study between 1971 and 1974 of presumably healthy individuals aged 1–74 years [120]. Serum changes can be influenced by dietary magnesium intake and albumin levels, but can also be affected by short term changes like day to day and hour to hour variability of the amount of magnesium absorbed and excreted through the kidneys [121]. Blood levels have been shown to increase in response to magnesium supplementation, but this does not signal that complete equilibrium has been established between blood and the nearly 100-fold larger body reservoir of magnesium. In fact, the much larger exchangeable pool of magnesium is more often called upon to augment blood levels to maintain a narrow range preferentially, which is a key reason why blood measurements can easily mask deficiency [122,123].
The tight control of magnesium serum levels, representing only 0.8% of total body stores (see Section 2.4), therefore serves as a poor proxy for the 99.2% of magnesium in other tissues that constitutes the body’s true magnesium status. Furthermore, this narrow serum range feeds the common perception of clinicians that magnesium levels rarely fluctuate, and therefore, are not indicative of the condition for which the blood tests are ordered. Therefore, practitioners are apt to order blood tests for magnesium infrequently, if at all, and if a magnesium level is in the patient chart, it is more often as part of a blood test panel and not purposely ordered to determine the magnesium status [89,124,125,126]. This contributes significantly to magnesium deficiency not being recognized as a modifiable nutritional intervention, and magnesium in general, being the neglected mineral that it is.
Red blood cells’ (RBC; erythrocyte and monocyte) magnesium levels are often cited as preferable to serum or plasma levels due to their higher magnesium content (0.5% vs. 0.3%, respectively). Some RBC studies report correlation to magnesium status particularly when subjects are placed on long-term (~3 months) magnesium replete or deplete diets. However, most studies using RBC magnesium endpoints do not satisfy this long-term design and have not been performed in nearly enough randomized clinical studies to be considered sufficiently robust or reliable (Table 1) [127,128,129]. In addition, the majority of RBC studies do not validate the method through inter-compartmental sampling (e.g., urine and muscle), challenging the claim that this test is a reliable representation of the large magnesium pool.”
Magnesium is a critical mineral in the human body and is involved in ~80% of known metabolic functions. It is currently estimated that 60% of adults do not achieve the average dietary intake (ADI) and 45% of Americans are magnesium deficient, a ...
Yes, an in-range value does not exclude some magnesium deficiency.
A low value, however, explicitly identifies low magnesium.
I am well aware.
Most of the cases regarding serum levels not being representative of body stores are in the elderly, long-term alcohol abusers, diabetics, and people with diseases that skew their calcium, magnesium, phosphorus and potassium levels.
For the average person, serum magnesium blood tests are reasonably accurate.
Magnesium supplementation can be carried out empirically.
As long as renal function isn't impaired and the rate at which magnesium is supplemented is not too fast, one can calculate the maximum body load of magnesium and supplement accordingly, taking into account type of magnesium, dosing, bioavailability, etc.
Magnesium is a critical mineral in the human body and is involved in ~80% of known metabolic functions. It is currently estimated that 60% of adults do not achieve the average dietary intake (ADI) and 45% of Americans are magnesium deficient, a ...
www.ncbi.nlm.nih.gov
“Once magnesium is absorbed it is distributed throughout the body for use and storage. Only 0.8% of magnesium is found in blood with 0.3% in serum and 0.5% in erythrocytes, with a typical total magnesium serum concentration between 0.65–1.0 mmol/L [89,90]. The rest is distributed in soft tissue (19%), muscle (27%), and bone (53%) (Figure 6) [89,90,91]. Up to one-third of the magnesium stored in bone is exchangeable [92], and while the total amount of magnesium stored in bone can change with age, bone remains the most significant area of stored and exchangeable magnesium.”
Which in most people is absolutely representative of body stores.
As you said, it's tightly regulated, meaning scientists have identified what serum levels correspond to body stores in most people.
Unless you're suffering from tetany, arrhythmias, weak muscles, tremor, nausea and vomiting, and you can add the rest of the symptoms of severe or significant magnesium deficiency, a week of oral supplementation at the correct dosages will fix you right up.
Otherwise, you need to get multi-gram iv infusions of magnesium sulfate
So I had an LTC years ago and can confirm the HPA axis theory. I had many tests done and my pregnenolone, testosterone levels were low and my saliva cortisol was blunted. Doing HCG+TRT+Preg supplementation and time worked for me and alleviated my anxiety.
I think the key is whether one has anhedonia though. HPA axis dysfunction alone will cause anxiety and low mood but not anhedonia in my experience. Anhedonia is typically going to be more than just a dysfunction of the HPA axis, like perhaps an alteration in allopregnanolone levels as well. I think the medication Zuranolone on the horizon could very well be an LTC cure.
As far as magnesium, the serum tests aren't that accurate. RBC Magnesium blood test is what you want to get to check the cellular level of Mg. There's more written about this in the book The Magnesium Miracle.
Well, it's funny you should say that because HPA axis hyperactivity meaning dysfunction is indicated in major depressive disorder. Anhedonia is one of the hallmarks of major depressive disorder.
The hypothalamic-pituitary-adrenal (HPA) axis is involved in the pathophysiology of many neuropsychiatric disorders. Increased HPA axis activity can be observed during chronic stress, which plays a key role in the pathophysiology of depression. Overactivity of the HPA axis occurs in major...
Which in most people is absolutely representative of body stores.
As you said, it's tightly regulated, meaning scientists have identified what serum levels correspond to body stores in most people.
Unless you're suffering from tetany, arrhythmias, weak muscles, tremor, nausea and vomiting, and you can add the rest of the symptoms of severe or significant magnesium deficiency, a week of oral supplementation at the correct dosages will fix you right up.
Otherwise, you need to get multi-gram iv infusions of magnesium sulfate
“In fact, the much larger exchangeable pool of magnesium is more often called upon to augment blood levels to maintain a narrow range preferentially, which is a key reason why blood measurements can easily mask deficiency”
I’m not sure what you’re not understanding about this. I even put it in bold.
BadooKing hit the nail on the head. It’s this method that you want to look at -> “As far as magnesium, the serum tests aren't that accurate. RBC Magnesium blood test is what you want to get to check the cellular level of Mg”
Whether it’s the HPA axis theory or mag deficiency doesn’t matter to me. I’m just trying to figure out what’s working.
“In fact, the much larger exchangeable pool of magnesium is more often called upon to augment blood levels to maintain a narrow range preferentially, which is a key reason why blood measurements can easily mask deficiency”
I’m not sure what you’re not understanding about this. I even put it in bold.
BadooKing hit the nail on the head. It’s this method that you want to look at -> “As far as magnesium, the serum tests aren't that accurate. RBC Magnesium blood test is what you want to get to check the cellular level of Mg”
I’m just going to put this to bed. I’m not going to try to convince you. Everyone else can read what has been said and decide for themselves.
Since 99% of the body's magnesium is stored in the bones, the muscles, and soft tissue; using your logic, red blood cell magnesium levels are not representative of the body's magnesium levels.
They're called biomarkers for a reason, except in certain specific cases they are reasonably representative.
Since 99% of the body's magnesium is stored in the bones, the muscles, and soft tissue; using your logic, red blood cell magnesium levels are not representative of the body's magnesium levels.
They're called biomarkers for a reason, except in certain specific cases they are reasonably representative.
Well, it's funny you should say that because HPA axis hyperactivity meaning dysfunction is indicated in major depressive disorder. Anhedonia is one of the hallmarks of major depressive disorder.
The hypothalamic-pituitary-adrenal (HPA) axis is involved in the pathophysiology of many neuropsychiatric disorders. Increased HPA axis activity can be observed during chronic stress, which plays a key role in the pathophysiology of depression. Overactivity of the HPA axis occurs in major...
Anhedonia is not there in every depressed individual though. I should also rephrase—if you have anhedonia yes there may be an alteration in HPA axis but solving that *alone* will probably not solve the anhedonia. In my LTC my main symptom was just anxiety and low mood, and I had HPA alterations on the DUTCH test.
Anhedonia is more to do with GABA-Glutamate and perhaps neurosteroids (some consider neurosteroids as part of HPA though, so if you do then yes it is related).
Recently, after COVID my body became super sensitive to alcohol and caffeine and I got HPA dysfunction again but my symptoms are way different in fact even worse than LTC as I have emotional blunting now, which I had none of back then. My HPA axis pregnenolone levels crashed in the beginning of this again and now they have recovered and I feel better but its still not resolved. Also my cortisol patterns are fine (including awakening response—I did the DUTCH test again which I recommend btw). I also found out I have SIBO. So at least for me it seems like blunting/anhedonia are separate from HPA axis.
Also its more likely the opposite of HPA hyperactivity but instead blunted cortisol response in LTC. That is similar to PTSD.
I recommend people see a hormone therapy specialist—not an endocrinologist—but HRT clinics or functional medicine docs. They can assess HPA.
By the way, high dose vit C infusions were also helpful for me in the middle lf an LTC. Mostly temporarily but theres something to it. I don’t think its fully placebo, there are anti inflammatory effects. Expensive though.
By the way, high dose vit C infusions were also helpful for me in the middle lf an LTC. Mostly temporarily but theres something to it. I don’t think its fully placebo, there are anti inflammatory effects. Expensive though.
That's interesting because I've always taken gram level doses of vitamin C multiple times per day, pretty much my entire life that I can remember.
I've never lost the magic and I used to roll multiple days per week every week for over a year and a half at one point. And then continued intermittently for the last 22 years.
That's interesting because I've always taken gram level doses of vitamin C multiple times per day, pretty much my entire life that I can remember.
I've never lost the magic and I used to roll multiple days per week every week for over a year and a half at one point. And then continued intermittently for the last 22 years.
Vit C pills are good but there was just something to the infusions where I felt refreshed. I'm sure part of it is placebo but the blood levels you get with IV are much higher. Vit C is pretty good for the HPA axis too.
Ketamine is the prototype for glutamate-based fast-acting antidepressants. The establishment of ketamine-like drugs is still a challenge and ascorbic …
www.sciencedirect.com
Another thing I think which predisposes one to HPA or neurosteroid issues is low cholesterol. My chol levels were always very low like 100, so something like MDMA could easily mess up the steroid cascade and neurosteroids too. I wonder what the chol levels are of the LTC sufferers
Also I tried AlloPregnanolone drops recently for my caffeine blunting issue and they were amazing temporarily. The first time it felt almost like MDMA itself, so I think there’s a connection and its not serotonin.
So I had an LTC years ago and can confirm the HPA axis theory. I had many tests done and my pregnenolone, testosterone levels were low and my saliva cortisol was blunted. Doing HCG+TRT+Preg supplementation and time worked for me and alleviated my anxiety.
I think the key is whether one has anhedonia though. HPA axis dysfunction alone will cause anxiety and low mood but not anhedonia in my experience. Anhedonia is typically going to be more than just a dysfunction of the HPA axis, like perhaps an alteration in allopregnanolone levels as well. I think the medication Zuranolone on the horizon could very well be an LTC cure.
As far as magnesium, the serum tests aren't that accurate. RBC Magnesium blood test is what you want to get to check the cellular level of Mg. There's more written about this in the book The Magnesium Miracle.
Vit C pills are good but there was just something to the infusions where I felt refreshed. I'm sure part of it is placebo but the blood levels you get with IV are much higher. Vit C is pretty good for the HPA axis too.
Ketamine is the prototype for glutamate-based fast-acting antidepressants. The establishment of ketamine-like drugs is still a challenge and ascorbic …
www.sciencedirect.com
Another thing I think which predisposes one to HPA or neurosteroid issues is low cholesterol. My chol levels were always very low like 100, so something like MDMA could easily mess up the steroid cascade and neurosteroids too. I wonder what the chol levels are of the LTC sufferers
Also I tried AlloPregnanolone drops recently for my caffeine blunting issue and they were amazing temporarily. The first time it felt almost like MDMA itself, so I think there’s a connection and its not serotonin.




 www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov






")