greengummybear
Bluelighter
- Joined
- Dec 23, 2014
- Messages
- 172
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6101a3.htmUnited States Centers for Disease Control and Prevention said: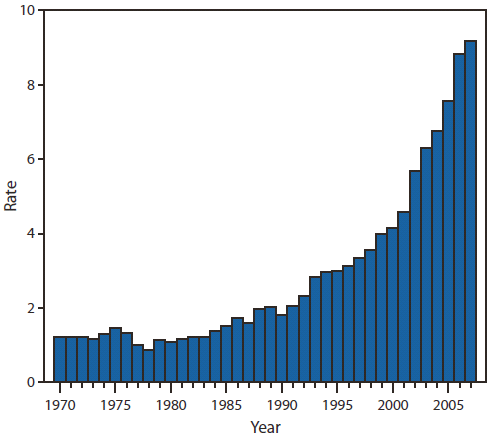
*
CDC Grand Rounds: Prescription Drug Overdoses — a U.S. Epidemic
This is another in a series of occasional MMWR reports titled CDC Grand Rounds. These reports are based on grand rounds presentations at CDC on high-profile issues in public health science, practice, and policy. Information about CDC Grand Rounds is available at http://www.cdc.gov/about/grand-rounds.
In 2007, approximately 27,000 unintentional drug overdose deaths occurred in the United States, one death every 19 minutes. Prescription drug abuse is the fastest growing drug problem in the United States. The increase in unintentional drug overdose death rates in recent years (Figure 1) has been driven by increased use of a class of prescription drugs called opioid analgesics (1). Since 2003, more overdose deaths have involved opioid analgesics than heroin and cocaine combined (Figure 2) (1). In addition, for every unintentional overdose death related to an opioid analgesic, nine persons are admitted for substance abuse treatment (2), 35 visit emergency departments (3), 161 report drug abuse or dependence, and 461 report nonmedical uses of opioid analgesics (4). Implementing strategies that target those persons at greatest risk will require strong coordination and collaboration at the federal, state, local, and tribal levels, as well as engagement of parents, youth influencers, health-care professionals, and policy-makers.
Overall, rates of opioid analgesic misuse and overdose death are highest among men, persons aged 20–64 years, non-Hispanic whites, and poor and rural populations. Persons who have mental illness are overrepresented among both those who are prescribed opioids and those who overdose on them. Further defining populations at greater risk is critical for development and implementation of effective interventions. The two main populations in the United States at risk for prescription drug overdose are the approximately 9 million persons who report long-term medical use of opioids (5), and the roughly 5 million persons who report nonmedical use (i.e., use without a prescription or medical need), in the past month (4). In an attempt to treat patient pain better, practitioners have greatly increased their rate of opioid prescribing over the past decade. Drug distribution through the pharmaceutical supply chain was the equivalent of 96 mg of morphine per person in 1997 and approximately 700 mg per person in 2007, an increase of >600% (6). That 700 mg of morphine per person is enough for everyone in the United States to take a typical 5 mg dose of Vicodin (hydrocodone and acetaminophen) every 4 hours for 3 weeks. Persons who abuse opioids have learned to exploit this new practitioner sensitivity to patient pain, and clinicians struggle to treat patients without overprescribing these drugs.
Among patients who are prescribed opioids, an estimated 80% are prescribed low doses (<100 mg morphine equivalent dose per day) by a single practitioner ( 7,8 ), and these patients account for an estimated 20% of all prescription drug overdoses (Figure 3). Another 10% of patients are prescribed high doses (≥100 mg morphine equivalent dose per day) of opioids by single prescribers and account for an estimated 40% of prescription opioid overdoses (9,10). The remaining 10% of patients are of greatest concern. These are patients who seek care from multiple doctors and are prescribed high daily doses, and account for another 40% of opioid overdoses (11). Persons in this third group not only are at high risk for overdose themselves but are likely diverting or providing drugs to others who are using them without prescriptions. In fact, 76% of nonmedical users report getting drugs that had been prescribed to someone else, and only 20% report that they acquired the drug from their own doctor (4). Furthermore, among persons who died of opioid overdoses, a significant proportion did not have a prescription in their records for the opioid that killed them; in West Virginia, Utah, and Ohio, 25%–66% of those who died of pharmaceutical overdoses used opioids originally prescribed to someone else (11–13). These data suggest that prevention of opioid overdose deaths should focus on strategies that target 1) high-dosage medical users and 2) persons who seek care from multiple doctors, receive high doses, and likely are involved in drug diversion. ...
*The War on Drugs began in the 1970s