


nAON
Bluelight Crew
Some of you may recognise this visual that has, for me at least, been rinsing its way through my facebook for the last few weeks, apparently showing that psilocybin increases connectivity and activity across discrete brain regions. [source = http://rsif.royalsocietypublishing.org/content/11/101/20140873.full.pdf+html]
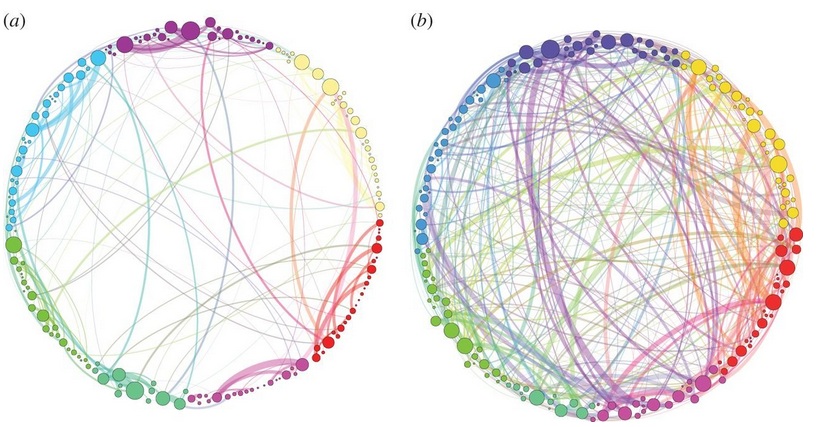
I have attempted to read the paper and failed miserably, too many equations and network-lingo for me. Could anyone here help explain this to me? How was this visual created, what does it show exactly, and what are the implications? How does it integrate into previous fMRI findings that show overall decreased connectivity in the brain on psilocybin?
I have attempted to read the paper and failed miserably, too many equations and network-lingo for me. Could anyone here help explain this to me? How was this visual created, what does it show exactly, and what are the implications? How does it integrate into previous fMRI findings that show overall decreased connectivity in the brain on psilocybin?


")