JTemperance
Bluelight Crew
- Joined
- May 15, 2016
- Messages
- 1,345
Yes, I should say that I was just thinking out loud and that I would not advise anyone to do something like that, nor would I do so myself, at least not until there was much better information on the issue.I'm not sure how effective this would be / how risky it could be.
My main worry is that wcs seems to cause total unresponsiveness, so somebody experiencing it wouldn't be able to treat themselves.
Second, I would be very conservative about reccomending treatments that will increase the severity of respiratory/cardiac depression. Slamming clonidine seems like it could seriously drop cardiorespiratory drive.
Honestly best advice i currently have (which is likely not super feasible) is don't use alone, and have a positive pressure bag mask so that the observer can force respiration. These can be bought online.
I admit it's frightening, though, so I do feel an urge to come up with some kind of strategy to mitigate the risk. Your advice re: positive pressure bag mask is well-taken, and since I'm lucky enough to have someone I can shoot with, it could be useful for me personally.
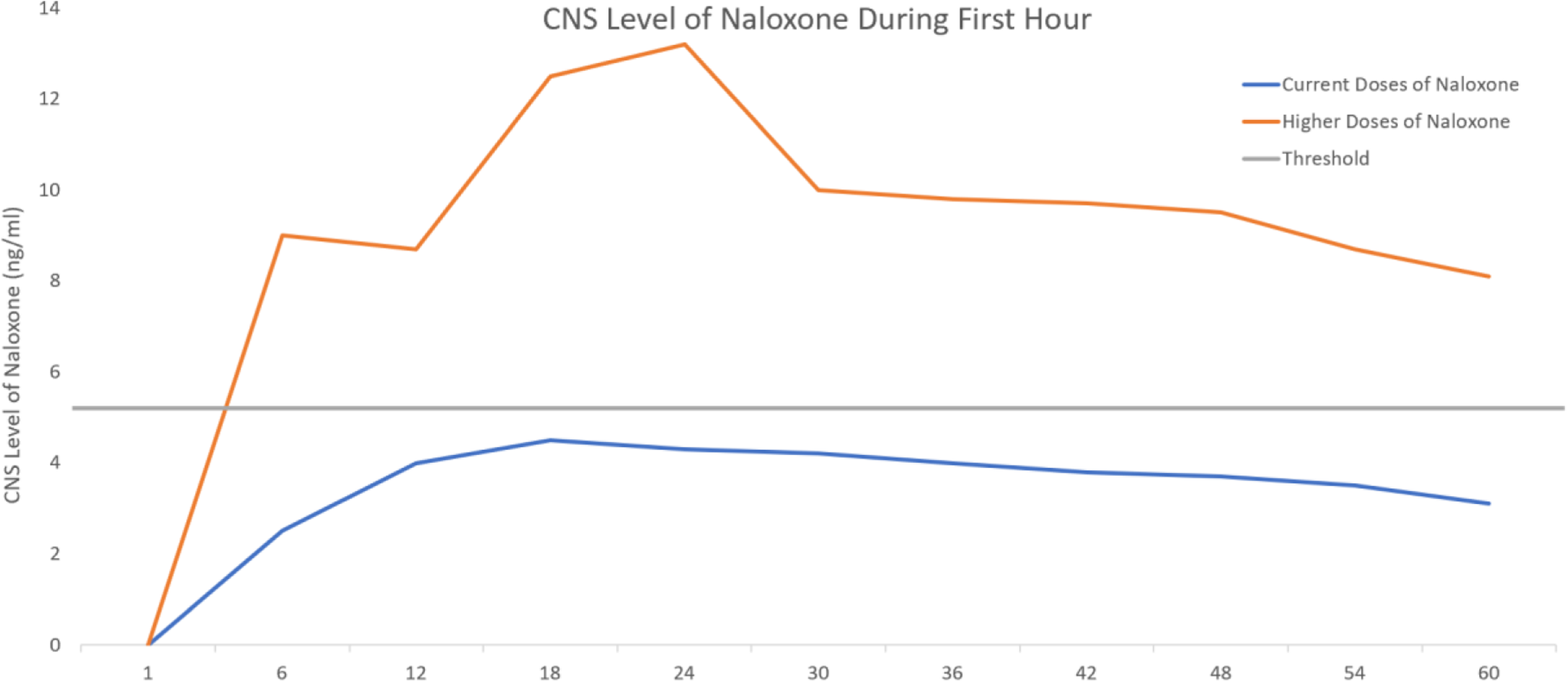
One other question I had was: how common do non-reversible (w/ Narcan) fentanyl "overdoses" appear to be? Is it something EMTs are encountering a lot out in the field?
Last edited: