dopamimetic
Bluelighter
- Joined
- Mar 21, 2013
- Messages
- 2,070
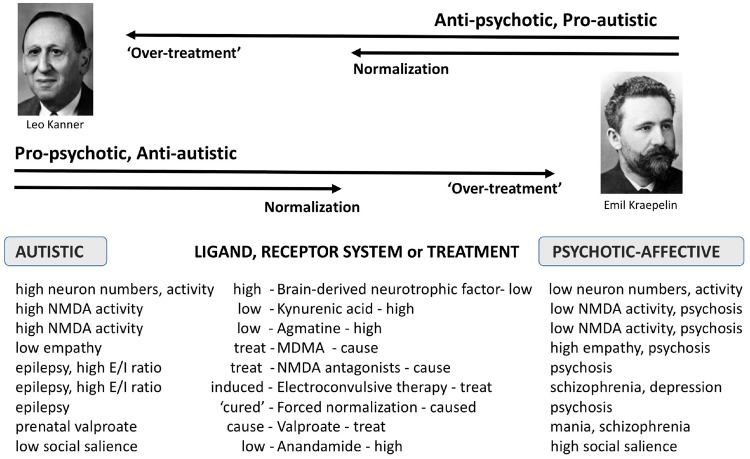
Just found this very interesting paper, not only contains a graph that indeed appears to confirm one of the more "strange" theories I developed in the past years but also other things around it. Indicates that autism spectrum disorders and psychosis are the opposite ends of NMDA receptor dysfunction/dysbalance, finally, while earlier papers always only covered the normal to psychosis part of the picture which confused me somewhat as my own experiences did not fit in this.
Also it's not just me, I know a (unfortunately just one) friend with confirmed Asperger's diagnosis and her experiences are much the same as mine. Just she tolerates DXM much better and chose it as her DOC while I tried my way through the arylcyclohexylamines and memantine, the latter being imho a very underrated substance that, together with venlafaxine, improves my condition by so much..
Sigma receptor isn't mentioned in the study but I would suggest from my "data" that agonism is good and antagonism (sertraline, haloperidol etc) is bad. Yay, even my old kynurenic acid is there. Agmatine is no surprise, but might it make an effective treatment?? Never thought about trying that. Had sarcosine but after horrible experiences with even low dosages of the hyped racetams (granted, not exactly the same, but made me vary about going pro-NMDA) I only tried little of it without any noticeable results. [shortly afterwards, my ex flushed all my chems]
Yeah, what do you think? Could NMDA antagonists, especially memantine in higher dosages (20-50mg) possibly combined with an antidepressant*, make a considerable anti-autistic medicine? It would fit with my impression that they are two-phasic, first improvement, then worsening again and psychotomimesis.. it always confused me that ketamine etc. are described as being psychotomimetic in healthy volunteers at low dosages etc..
* memantine alone didn't cut it for me, got depressed and anxious after the initial stimulation faded away. venlafaxine alone didn't either, it helps but there's always something missing. together it's the best aid I known, besides that ominous 4,4'-dimethylaminorex of which I'd almost bet it'd show some NMDA antagonism too.
How does this fit with earlier theories, like too much endorphines and GABAergic inhibition? I know that NMDA antagonism is associated with less inhibition (check) and lowered tolerance to opioids (?? - yeah, even memenatine is strong enough to get me off 200mg morphine.. seems oppositing but morphine != endorphines and oppositing to almost everybody, opioids can be heavily psychotomimetic for me too).
Also it's not just me, I know a (unfortunately just one) friend with confirmed Asperger's diagnosis and her experiences are much the same as mine. Just she tolerates DXM much better and chose it as her DOC while I tried my way through the arylcyclohexylamines and memantine, the latter being imho a very underrated substance that, together with venlafaxine, improves my condition by so much..
Sigma receptor isn't mentioned in the study but I would suggest from my "data" that agonism is good and antagonism (sertraline, haloperidol etc) is bad. Yay, even my old kynurenic acid is there. Agmatine is no surprise, but might it make an effective treatment?? Never thought about trying that. Had sarcosine but after horrible experiences with even low dosages of the hyped racetams (granted, not exactly the same, but made me vary about going pro-NMDA) I only tried little of it without any noticeable results. [shortly afterwards, my ex flushed all my chems]
Yeah, what do you think? Could NMDA antagonists, especially memantine in higher dosages (20-50mg) possibly combined with an antidepressant*, make a considerable anti-autistic medicine? It would fit with my impression that they are two-phasic, first improvement, then worsening again and psychotomimesis.. it always confused me that ketamine etc. are described as being psychotomimetic in healthy volunteers at low dosages etc..
* memantine alone didn't cut it for me, got depressed and anxious after the initial stimulation faded away. venlafaxine alone didn't either, it helps but there's always something missing. together it's the best aid I known, besides that ominous 4,4'-dimethylaminorex of which I'd almost bet it'd show some NMDA antagonism too.
How does this fit with earlier theories, like too much endorphines and GABAergic inhibition? I know that NMDA antagonism is associated with less inhibition (check) and lowered tolerance to opioids (?? - yeah, even memenatine is strong enough to get me off 200mg morphine.. seems oppositing but morphine != endorphines and oppositing to almost everybody, opioids can be heavily psychotomimetic for me too).
")