Feretile
Bluelighter
- Joined
- Feb 2, 2022
- Messages
- 361
Loperamide has a 2-phase dose/response curve, has roughly 1/40th of the mu affinity of codeine and the specific dose at which the ABC binding cassette is overcome and the drug reaches it's second phase dose-response.
Loperamide is an extreme example of a compound removed from the brain by Pgp efflux (efflux ratios ranging from 6.5 to 9.9). UNTIL the user consumes a sufficient amount of the drug to overcome the Pgp, almost none of it will reach the brain. This dose-range is considered to be the first phase.
The blood-brain barrier (BBB) is a network of highly selective cells that protect the brain from toxic insults.1 The ATP binding cassette (ABC) transporter P-glycoprotein (Pgp) is highly expressed on the apical surface of the BBB. Pgp is a highly promiscuous protein that effluxes a structurally and chemically diverse range of compounds away from the brain into the bloodstream. While this function is critical for neurohomeostasis and for preventing the penetration of toxic insults, Pgp’s role at the BBB prevents the entry of many neurotherapeutics and represents a formidable hurdle to drug development. Over the last three decades, considerable effort has been made to improve penetration of drugs by inhibiting Pgp, but this has been unsuccessful in the clinic because of unforeseen toxicity. As a result, there has been considerable interest in the pharmaceutical industry to identify the molecular features of drugs that drive Pgp-mediated transport.
The dose-response in the second phase has not been tested scientifically in any animal, let alone a human study. All I DO know is that there are regular reports of people taking around 200 mg to manage the symptoms of opioid abstinence syndrome (does generic loperamide come in 100 capsule lots in the US as 200mg is common). These same people have ended up as medical emergencies when they increased the dose by less than 20%. There have been 19 serious loperamide poisonings in the UK (5 fatal). The death-toll in the US isn't available (although someone could sit their & find death toll in each state - a truly useful if boring job)
Ones opiod tolerance will have NO effect in the first phase of dose/response BUT is a very shallow slope because while plasma levels rise, the Pgp ensures that levels in the brain do not. Given the LOW and I mean LOW activity of loperamide, even a naïve user will feel almost no opioid effects and in tolerant users their will certainly be no effect.
Of course, since the user has managed to overcome the Pgg of their BBB, all manner of other toxins will enter the brain so the cause of injury/death are hard to qualify. I am of the opinion that the self-destructive martians who take handfuls of loperamide are those satisfied with ANY subjective alteration of reality bestowed on them by drugs.
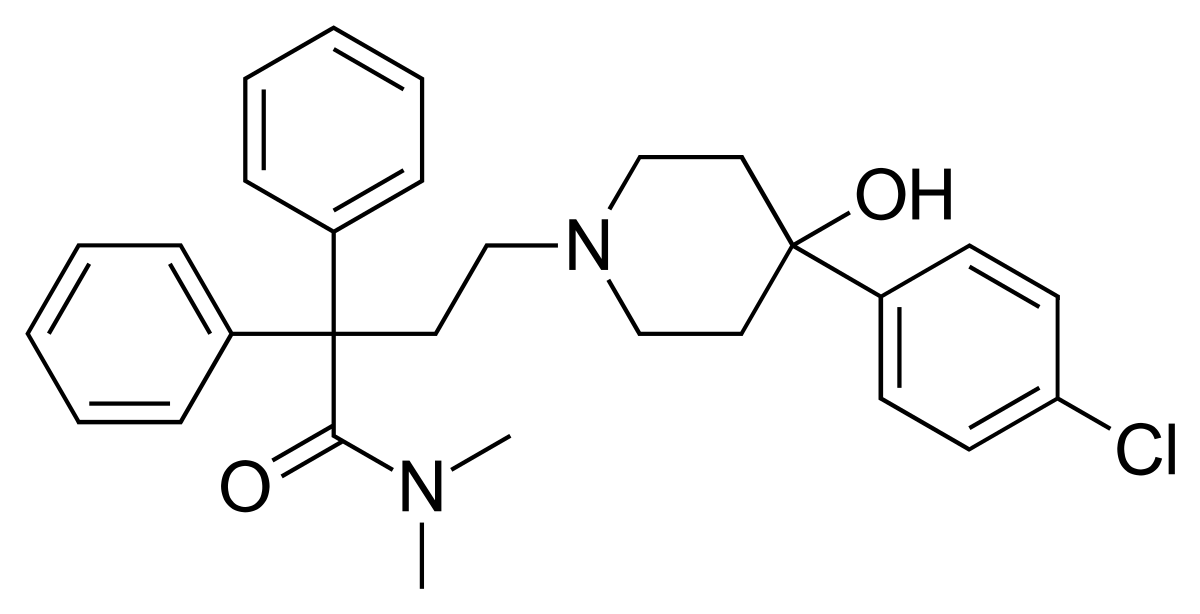
Many amateur chemist have proposed numerous ways to alter loperamide to make it into a potent opioid. Well, US Patent 3714159 covers loperamide & related compounds but whatever modification is suggested, the LogP of loperamide is just too high. Janssen also discovered dextromoramide and that study showed that for alkyl amides, only a pyrrolidine will produce strong analgesia (see dextromoramide).
Of course, if one could remove the p-Cl, demethylate the amide & form a (m)ethyl ester with the quaternary -OH..... THEN the LogP would be low enough and you would be left with an opioid with all the kick of codeine.
 en.wikipedia.org
en.wikipedia.org
Put simply - ir's much less work to make an opioid from scratch than to attempt to manipulate loperamide.
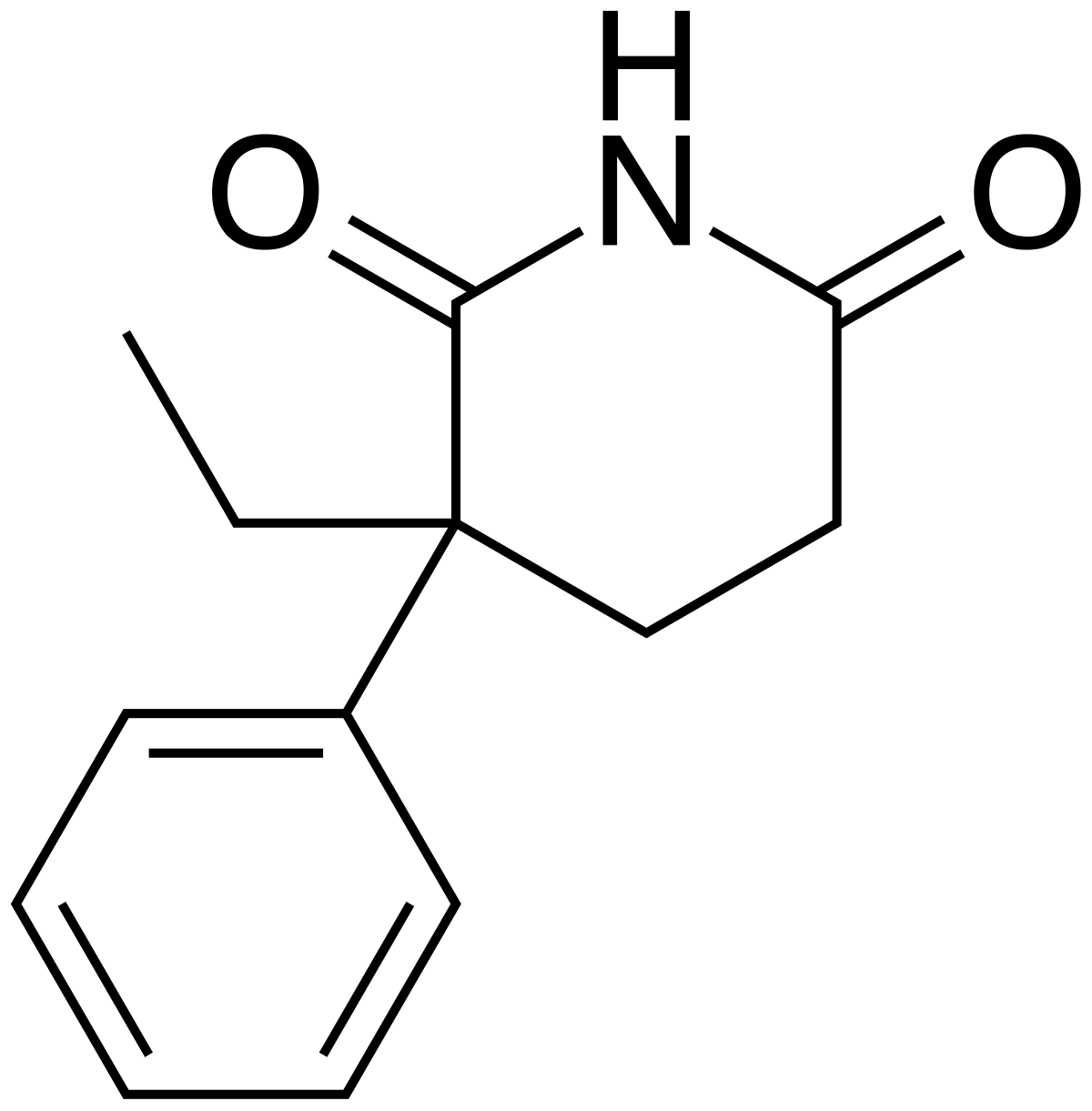
But if you want 'out of the box' thinking, why not produce the isopropyl analogue of glutethimide? It induces the CYP2D6 liver enzyme and so rather than the body converting approximately10% of codeine--->morphine, hydrocodone--->hydromorphone & oxycodone--->oxymorphone, it converts rather more than 90%.
 en.wikipedia.org
en.wikipedia.org
Now, glutethimide has a chiral centre and the 2 enanthiomers are metabolised via different pathways but if only 1 isomer is responsible for CYP2D6 induction, a chiral synthesis sounds a good idea.. It came as 250mg & 500mg tablets & users would take 2 along with 3 Tylanol 4s.
While Doriden (glutethimide) only uses a 2-step synthesis, it's still not going to be worth much, is it? Well, apart from someone who has a 160mg/day OxyContin habit - capsules with just 5mg of oxycodone & 250mg of glutethimide will happily replace one dependence with another (ALWAYS a clever move). As long as a criminal can obtain a prodrug that is so thanks to a phenylmethyl ether, they are in business.
Just my little idea of how much worse things can get. Oh, BTW, NO, glutethimide will nor make loperamide stronger!
Loperamide is an extreme example of a compound removed from the brain by Pgp efflux (efflux ratios ranging from 6.5 to 9.9). UNTIL the user consumes a sufficient amount of the drug to overcome the Pgp, almost none of it will reach the brain. This dose-range is considered to be the first phase.
The blood-brain barrier (BBB) is a network of highly selective cells that protect the brain from toxic insults.1 The ATP binding cassette (ABC) transporter P-glycoprotein (Pgp) is highly expressed on the apical surface of the BBB. Pgp is a highly promiscuous protein that effluxes a structurally and chemically diverse range of compounds away from the brain into the bloodstream. While this function is critical for neurohomeostasis and for preventing the penetration of toxic insults, Pgp’s role at the BBB prevents the entry of many neurotherapeutics and represents a formidable hurdle to drug development. Over the last three decades, considerable effort has been made to improve penetration of drugs by inhibiting Pgp, but this has been unsuccessful in the clinic because of unforeseen toxicity. As a result, there has been considerable interest in the pharmaceutical industry to identify the molecular features of drugs that drive Pgp-mediated transport.
The dose-response in the second phase has not been tested scientifically in any animal, let alone a human study. All I DO know is that there are regular reports of people taking around 200 mg to manage the symptoms of opioid abstinence syndrome (does generic loperamide come in 100 capsule lots in the US as 200mg is common). These same people have ended up as medical emergencies when they increased the dose by less than 20%. There have been 19 serious loperamide poisonings in the UK (5 fatal). The death-toll in the US isn't available (although someone could sit their & find death toll in each state - a truly useful if boring job)
Ones opiod tolerance will have NO effect in the first phase of dose/response BUT is a very shallow slope because while plasma levels rise, the Pgp ensures that levels in the brain do not. Given the LOW and I mean LOW activity of loperamide, even a naïve user will feel almost no opioid effects and in tolerant users their will certainly be no effect.
Of course, since the user has managed to overcome the Pgg of their BBB, all manner of other toxins will enter the brain so the cause of injury/death are hard to qualify. I am of the opinion that the self-destructive martians who take handfuls of loperamide are those satisfied with ANY subjective alteration of reality bestowed on them by drugs.
Many amateur chemist have proposed numerous ways to alter loperamide to make it into a potent opioid. Well, US Patent 3714159 covers loperamide & related compounds but whatever modification is suggested, the LogP of loperamide is just too high. Janssen also discovered dextromoramide and that study showed that for alkyl amides, only a pyrrolidine will produce strong analgesia (see dextromoramide).
Of course, if one could remove the p-Cl, demethylate the amide & form a (m)ethyl ester with the quaternary -OH..... THEN the LogP would be low enough and you would be left with an opioid with all the kick of codeine.
Loperamide - Wikipedia
Put simply - ir's much less work to make an opioid from scratch than to attempt to manipulate loperamide.
But if you want 'out of the box' thinking, why not produce the isopropyl analogue of glutethimide? It induces the CYP2D6 liver enzyme and so rather than the body converting approximately10% of codeine--->morphine, hydrocodone--->hydromorphone & oxycodone--->oxymorphone, it converts rather more than 90%.
Glutethimide - Wikipedia
Now, glutethimide has a chiral centre and the 2 enanthiomers are metabolised via different pathways but if only 1 isomer is responsible for CYP2D6 induction, a chiral synthesis sounds a good idea.. It came as 250mg & 500mg tablets & users would take 2 along with 3 Tylanol 4s.
While Doriden (glutethimide) only uses a 2-step synthesis, it's still not going to be worth much, is it? Well, apart from someone who has a 160mg/day OxyContin habit - capsules with just 5mg of oxycodone & 250mg of glutethimide will happily replace one dependence with another (ALWAYS a clever move). As long as a criminal can obtain a prodrug that is so thanks to a phenylmethyl ether, they are in business.
Just my little idea of how much worse things can get. Oh, BTW, NO, glutethimide will nor make loperamide stronger!


