

sekio
Bluelight Crew
So like most good chemists I'm always thinking about similarities. I remembered the old legend of, people on PCP are superhuman and able to lift cars, they get crazy aggressive, etc, and the like. I thought about its weird possible neuroregenerative processes. I also noted the fact that both arylcyclohexylamines and steroids are bulky, multicyclic compounds with at least one aromatic center and some little polar bits as decorations.
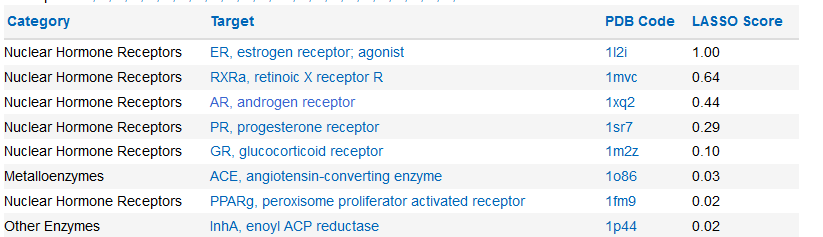
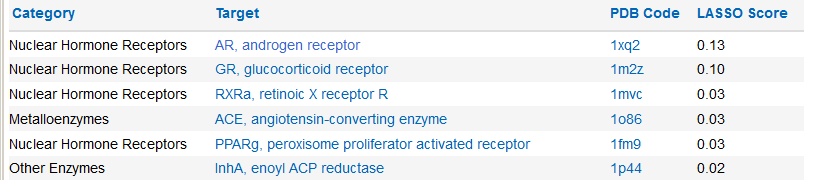
The first spot I go is to Chemspider, cause it has this LASSO thing, which predicts protein affinities. Here's what comes up.
Phencyclidine
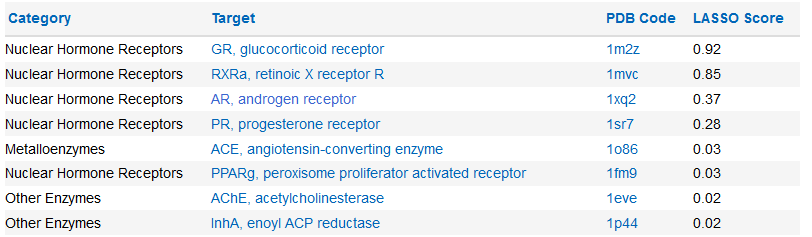
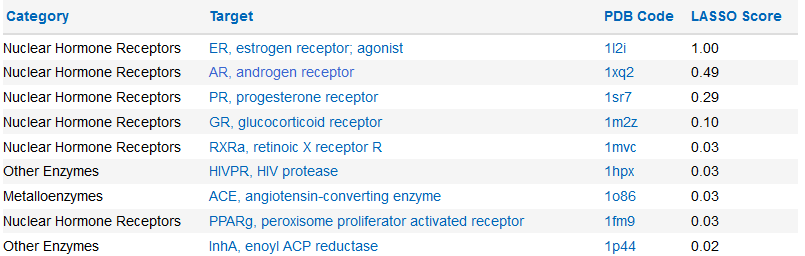
PCE
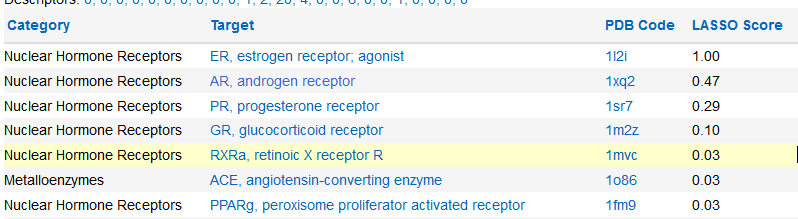
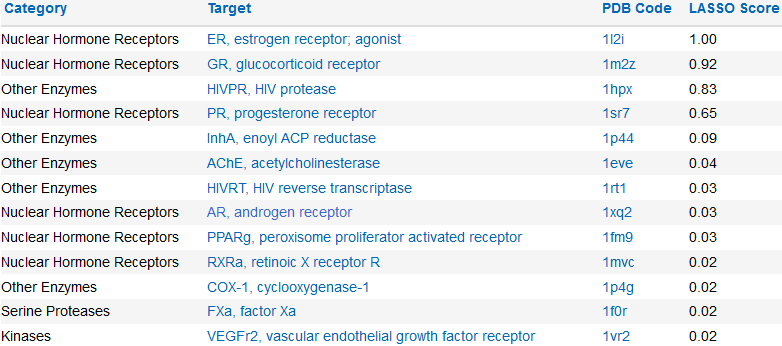
3-HO-PCP
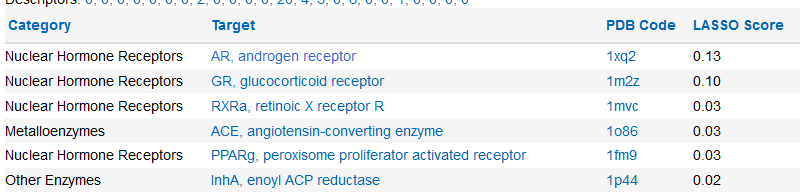
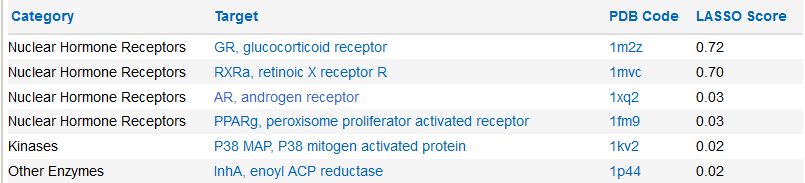
3-MeO-PCP
4-MeO-PCP
4'-OH-PCP
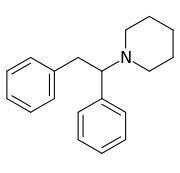
Diphenidine
(s)-Ketamine
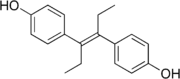
So... this is interesting. I know that stuff like tamoxifen and diethylstilbestrol kind of remind me of diphenidine.
Could this explain some of the ... strange effects of PCP and its analogs? Is this a red herring? Does Ashy Larry have bitch tits from smoking sherm? Does getting whacked on methoxy-diphenidine cure breast cancer?
The first spot I go is to Chemspider, cause it has this LASSO thing, which predicts protein affinities. Here's what comes up.
Phencyclidine
NSFW:
PCE
NSFW:
3-HO-PCP
NSFW:
3-MeO-PCP
NSFW:
4-MeO-PCP
NSFW:
4'-OH-PCP
NSFW:
Diphenidine
NSFW:
(s)-Ketamine
NSFW:
So... this is interesting. I know that stuff like tamoxifen and diethylstilbestrol kind of remind me of diphenidine.
Could this explain some of the ... strange effects of PCP and its analogs? Is this a red herring? Does Ashy Larry have bitch tits from smoking sherm? Does getting whacked on methoxy-diphenidine cure breast cancer?
Last edited:



") I don't know how much about these horror stories is true, but with reasonable dosing all the arylcyclohexylamines I know of were manageable (and each fascinating in its own way), including 3-MeO-PCP. The diphenylethylamines might be another thing though.
I don't know how much about these horror stories is true, but with reasonable dosing all the arylcyclohexylamines I know of were manageable (and each fascinating in its own way), including 3-MeO-PCP. The diphenylethylamines might be another thing though.