I found the following text (I'm not sure if I'm allowed to mention the forum):
Benzodiazepines vary in lipid solubility <abbreviated>
Benzodiazepine pKa
Bromazepam 11.0
Clonazepam 10.5 (1-position)
1.5 (4-position)
Diazepam 3.3
Flunitrazepam 1.8
Flurazepam 8.2
Lorazepam 11.5
Medazepam 6.2
Nitrazepam 10.8
Oxazepam 1.8
Prazepam 3.0
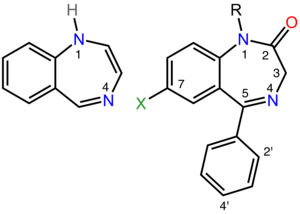
pKa is mentioned. I'm not familiar with this regarding lipid solubility. Also the '1 position' of clonazepam has a value of 10.5, and the '4' position has a value of 1.5.
So, how is the pKa relevant in this context ? And what is this about the '1' position, and the '4' position' ?
I was trying to find information about the lipophilicity of clonazepam, can someone help me make sense of these two values for this drug ?
Benzodiazepines vary in lipid solubility <abbreviated>
Benzodiazepine pKa
Bromazepam 11.0
Clonazepam 10.5 (1-position)
1.5 (4-position)
Diazepam 3.3
Flunitrazepam 1.8
Flurazepam 8.2
Lorazepam 11.5
Medazepam 6.2
Nitrazepam 10.8
Oxazepam 1.8
Prazepam 3.0
pKa is mentioned. I'm not familiar with this regarding lipid solubility. Also the '1 position' of clonazepam has a value of 10.5, and the '4' position has a value of 1.5.
So, how is the pKa relevant in this context ? And what is this about the '1' position, and the '4' position' ?
I was trying to find information about the lipophilicity of clonazepam, can someone help me make sense of these two values for this drug ?
") : would you happen to know (of a source) giving the (relative affinity) of various benzodiazepines to the various GABAA subunits ? Clonazepam and diazepam in particular.
: would you happen to know (of a source) giving the (relative affinity) of various benzodiazepines to the various GABAA subunits ? Clonazepam and diazepam in particular.