Nagelfar
Bluelight Crew
- Joined
- Nov 23, 2007
- Messages
- 2,527
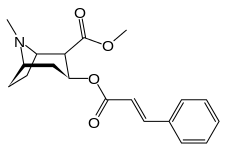
Well, it's up in the air whether cinnamoyl-cocaine is active or not; but things lean to it having gone under the radar being another active coca plant alkaloid:
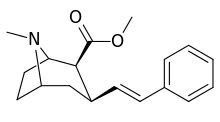
i.e.
The styrene is definitely active, and more potent than cocaine by more than forty-fold
I'd say highly possible, the naphthyl is your best bet just because of how long the linkage is getting.
As for the forward nitrogen, it's in a bit of a no-mans-land from previous SAR I've seen tested, but this for example:
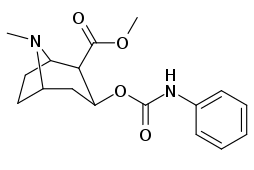
...is a functional ligand.
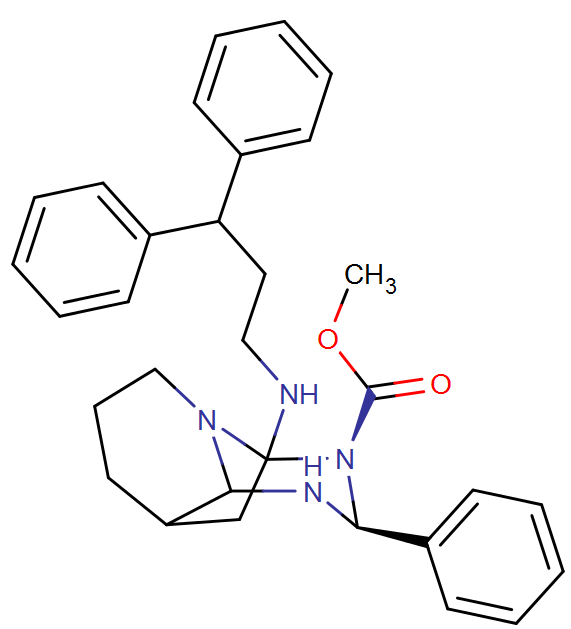
Makes me think of the SoRI-20041 phenyltropane hybrid, if that nitrogen works:
i.e.
The styrene is definitely active, and more potent than cocaine by more than forty-fold
I'd say highly possible, the naphthyl is your best bet just because of how long the linkage is getting.
As for the forward nitrogen, it's in a bit of a no-mans-land from previous SAR I've seen tested, but this for example:
...is a functional ligand.
Makes me think of the SoRI-20041 phenyltropane hybrid, if that nitrogen works:
Last edited: