'Hexen' makes me think of a term meaning 'accursed' in germanic tongues, as in 'hexenwulfen', curse-wolf or spell-wolf, someone cursed by another to transform into a werewolf. An omen of fucked up to come?

Although, although at first I dismissed 'hexen' (agreed its a fucking dog turd of a name, sounds too close to 'hexene' for somebody not to start selling that particular olefin on the street to/by/both-morons. Cyclohexene if they are smarter morons than the average prize pillock but not by much. Just enough to tie themselves in a mental knot, so to speak) as looking like it would be a humongous turd. I'd certainly expect that from the amphetamine version, but it seems cathinones are quite a bit more different than I thought at first after reading up on their pharmacology more. I'd have thought a big dirty great branched sidechain like that would have sounded the death knell for the substance and carved the word 'wankmeister' on its scrotum with a scalpel carved from its own asshole-bone and with a handle made from tanned dog dick leather....but hmm....maybe not. Looks like there be more than one way to skin a cat, so to speak.
Certainly, some similar branched cathinones look very interesting, in quite the unusual way, unique in fact as far as is definitively proven, namely PPAP, and BPAP, the benzofuranyl analog of the former, the PPAP being 1-phenyl-2-propylaminopentane, an amphetamine-like compound with a most unusual sidechain, and likewise unusual mode of action. Most psychostimulants act via one of two mechanisms, at least, directly acting ones, that work on the dopaminergic pathways themselves, dopamine releasers, and reuptake inhibitors* (*it now seems with more recent research that some of the reuptake inhibitors are in fact inverse agonists of the dopamine transporter rather than simple blockers, which has been suggested to explain why some ligands which occupy and block DAT, the dopamine transporter, of the phenyltropane family, related to cocaine are euphoric and highly rewarding, whilst others are not, the euphoric ones being those that reverse the action of DAT causing the synaptic terminal to spit out dopamine and prevent its reuptake whilst the non-euphorigenic ones institute a more simple blockade of reuptake from the synapse)
The releasers are those with action more similar to amphetamines, and they act to induce a massive release, although without so much effect on preventing its being reuptaken into the cytoplasm once spat forth into the synaptic cleft to act upon receptors and of course induce the subsequent consequences of such binding and activity within the neurons, according to receptor type, location and intracellular pathways, ergo also function, such as reward, in the nucleus accumbens/striatum, and in the substiantia nigra, inhibitory control over voluntary motor control.
They cause a much greater peak rise in DA (dopamine) levels in the synaptic cleft (space between two neurons where synaptic terminals of each branch out and connect to form the synapse, the space between being where neurotransmitters are released, typically by the presynaptic neuron, although in the case of the endocannabinoid system the direction of signalling is retrograde, the postsynaptic terminal sending feedback messages to mediate levels of neuronal excitability tonically) than do the DARIs (DopAmine Reuptake Inhibitor-DARI for short), which don't all seem to actively release DA, some as said, blocking transport back into the cell that released it, for repackaging into synaptic vesicles, the little intracellular compartments that serve for release of quantities of neurotransmitters, and thence recycling, as opposed to their other fate, catabolic enzymes like monoamine oxidases (MAO-a, MAO-b for noradrenaline/serotonin favouring and dopamine-favouring respectively, monoamine-breakdown enzymes) which destroy the same neurotransmitters rather than recycle them)
BPAP and PPAP are different, very much so, in that rather than either directly acting to cause the cell to dump out its reservoirs of dopamine, noradrenaline and serotonin (the three classic monoamines) or serving to prevent reuptake of, and thus cause a buildup of these, but to a lesser peak extent than the releasers, these two oddball and intriguing little fellas, is to act tonically rather than phasically, sort of like setting the gain on an amplifier, both of these unique drugs act in a way that results in, for a given stimulus, that would normally release one or more of these monoamine neurotransmitter types, rather than a simple dump of, or blockade of their being removed from activity (release and reuptake, respectively) that given stimulus to neurotransmitter release, when it occurs whilst the influence of PPAP or BPAP is in action to modulate the process, a larger quantity of neurotransmitter is released on a per-stimulus basis, so overall monoamine release is kicked up a notch, but only in response to events, be they naturally occuring sans the action of an external drug, or to potentiate also the activity of monoaminergic drugs.
Not sure if they affect directly acting receptor agonists (for example dopamine agonists such as pramipexole, ropinirole, some of the ergot alkaloids, adrenergic agonists (and autoreceptor antagonists, same goes for autoreceptors for other neurotransmitters, an autoreceptor being a receptor that when agonized, causes increase of transmitter release for that neurotransmitter, and an antagonist or too high levels of the neurotransmitter activate the autoreceptor and block neurotransmitter release, a good example being clonidine, an adrenergic alpha2 receptor agonist, or their relatives tizanidine, guanfacine and lofexidine, at least clonidine and lofexidine are used to help treat the hyperactivity of the sympathetic nervous system and adrenergic overactivity, in opioid withdrawal, as well as in clonidines case, and guanfacine in the US although guanfacine is unavailable in the UK, for blood pressure control in treating hypertension, tizanidine being a potent and effective muscle relaxer, I take it for some nerve damage that came as a result of getting my leg fucked up, and clonidine also, which I use as essentially a prophylactic against one of the downsides to being autie, namely, overloading, sensorily and as a result, physically. Overloads blow ass big time, hard to explain if you don't have to deal with them personally but think of it as a sensory input-invoked 'blue screen of death' mixed with WWII era shell-shock, that fuck, breed a bastard child and have said bastard child kick you in the face, and in the nuts simultaneously. Repeatedly. Usually when you're under the most stress and want it least, although often you get through the acute event and then when you really need to relax, and get your downtime, it sneaks up and kicks you in the balls and face at the same time when you've just metaphorically speaking, closed your eyes and begun to doze off in the time your comfiest. Just to be a total cunt.
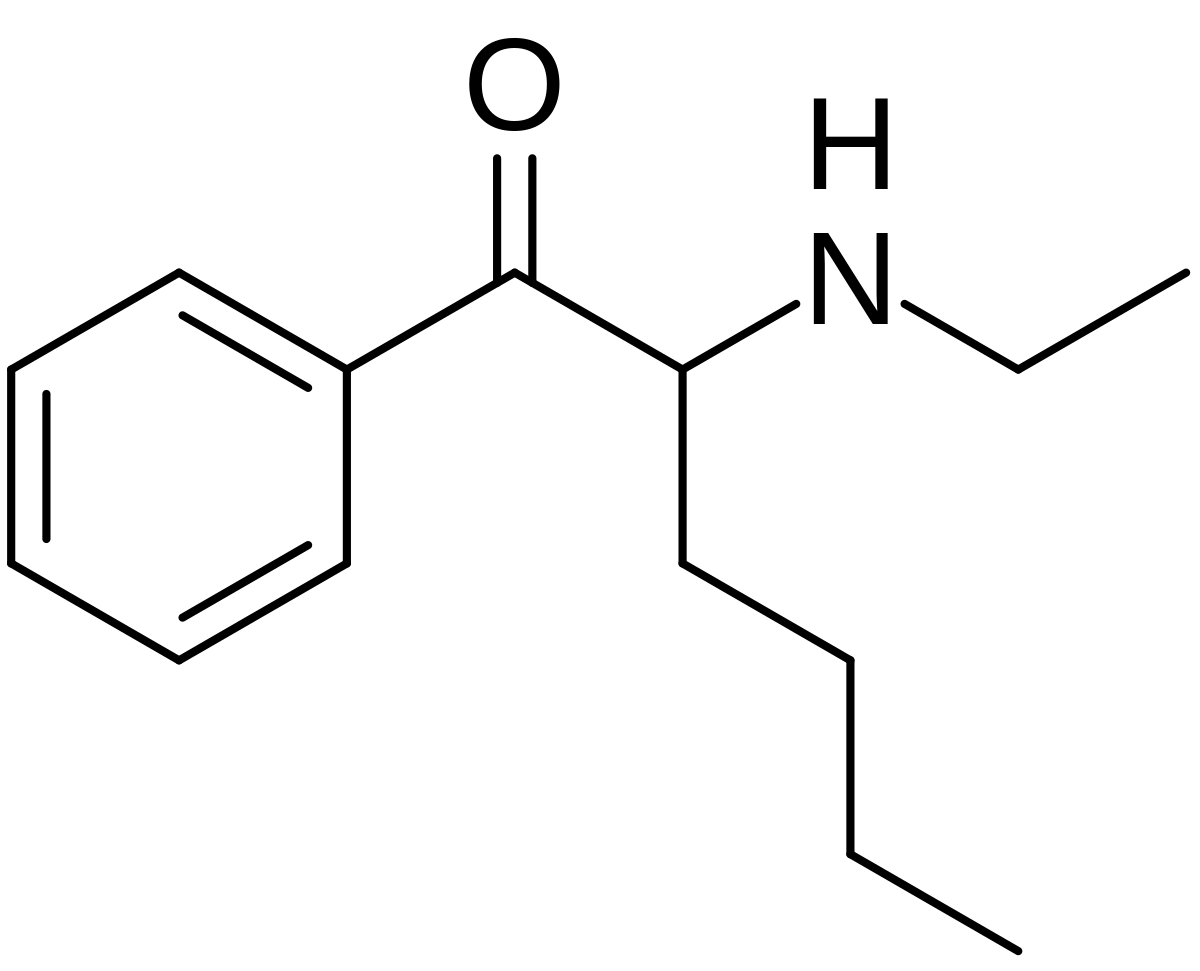
With a structure like the abysmally named 'hexen', wonder if it has any action of that kind.
I'd love to know. And love to try PPAP/BPAP and the two with a monoaminergic DA/NA releaser/reuptake inhibitor like meth, amphetamine, N-ethylamphetamine etc. or cocaine/methylphenidate/ethylphenidate respectively, and separately and together to boot, some of my rx'd pramipexole.
Unusual sidechain, looks more interesting than I thought at first given reports.

")