Weltmeister
Bluelighter
- Joined
- Oct 23, 2015
- Messages
- 231
Using them weekly (or even more) will probably bring about mental health problems anyway


N&PD Moderators: Skorpio | someguyontheinternet

Using them weekly (or even more) will probably bring about mental health problems anyway
Using them weekly (or even more) will probably bring about mental health problems anyway
It is my opinion that the use of psychedelic 5-ht2b agonists is safe when taken at most weekly.
However, i would NEVER use them more than once week!
There are a number of misstatements and factually incorrect information in your post."Psilocybin is not cardiotoxic due to 5ht2B agonism unless combined with MAO-A inhibitors or taken daily. Usually when drugs have high binding affinity for receptors and you take a high dose OR you get excess serotonin release due to both dual action of 5HT releasing and MAO-inhibitor action ( like cathinones or some research chemicals ). Often you get a cascade reaction - when high levels of neurotransmitters are released due to one receptor another one gets triggered/activated . This is why you have different effects at different dosages.
5HT2B affinity of psilocybin is too low to pose any threat to health. 5HT2B receptor however prevents or decrease serotonin syndrom, that is why people don't get serotonin syndrom from research chemicals unless they thake MAO-inhibitor or anti-depressants along with drugs.
You have to compare to other drugs like research chemicals for example benzofurans like 5-APB and 6-APB are releasers , reuptake inhibitors and have Monoamine oxidase inhibition activity. 6-APB has 5HT2B 3.5 or 3.7 ki value. That one point difference is huge when translated to micromolar saturation between neurons and synapses. Recalling from my head LSD had about around 1 ki value for almost all targeted 5HT receptors which is huge. Psilocybin binds to Serotonin transporters(SERT) and basically bumping endogenous monoamines of SERT, this is pretty much the same mechanism of SSRI.
All the compounds in psilocybin mushrooms are metabolized rather quickly but because it binds to SERT you have a pretty long subjective half-life of the effects. oral passage 163±64 minutes is about the normal half life for psilocybin. That doesn't translate to the 6 hours of effects people feel. If you get some research chemicals with a a half life of 2 hours and are purely releasers, you will stop feeling anything after those 2 hours. Normally it would be about 4 hours but due to downregulation the other half won't really have an effect. Also with psilocybin you have downregulation ( tolerance) so in theory you shouldn't peak after 3 hours.
When it binds to the SERT the SERT will eventually be broken down by MAO-A displacing the psilocybin from the SERT , however if you take MAO-A inhibitors, transporters won't be broken down resulting in more transport across the synaptic cleft. Thus the psilocybin you take only a small fraction will be transported across the synaptic cleft. Taking a MAO-A inhibitor like syrian rue will approximately result in a 3x to 4x increase of psilocybin forwarded to the synapses ( thus resulting in stronger 5HT2B receptor activation. The more Psilocybin reaches the receptors in the synaps the more this 5HT2B receptor will be activated. Also psilocybin has little A1 and A2 affinity. LSD is not a releaser of 5HT but also binds to SERT.
The normal dose of psilocybin will not result in for example fibrosis of heartvalves. The saturation is just too low and the half life too short. You cannot redose psilocybin over and over like research chemicals due this mechanism.Binding to A1 and A2 ( adrenergic ) receptors also cause sudden heart failure , hyperthrophy and myraid of other problems due to overstimulation of the parasympathic nerves. LSD has pretty strong affinity for dopamine and adrenergic receptors which probably would the main cause of cardiotoxicity.
Fenfluramine is a very potent 5HT2B agonist and its metabolite is also such agonist , it is both a releaser ( cause vesicles or boutons to release 5HT or other mono amines) and reuptake inhibitor ( causing transporters not to reuptake 5HT back into the neuron). Fenfluramine is cardiotoxic as hell because of this dual or triple mechanism, 5-APB and 6-APB ( triple mechanism) are probably very cardiotoxic as well because it also cause depletion of serotonin in vesicles. Psilocybin does not cause depletion because it only binds to transporters thus resulting in lower 5HT saturation than potent releasers i described before, psilocybin mimics serotonin on the transporters. It just not comes down to pure affinity values.
If you use a releaser which depletes the vesicles storing mono amines like serotonin, once the vesicle gets depleted or near depletion it gets destroyed/deleted - this is especially the case when you use a reuptake inhibitor and/or MAOI because serotonin gets only released and forwarded , not moved back into the neuron. Psilocybin mimics serotonin and binds to a transporter instead of emptying the vesicles( mono amine or 5HT storage. Re uptake inhibtors do not cause empyting and deletion of storage vesicles they only cause a lower density of certain receptors on long term due to downregulation. Drugs that depletes vesicles like most research chemicals cause a increase in receptor density probably because after drug use you have both 1. downregulation and 2. less serotonin coming off vesicles due to deletion of boutons/vesicles and 3. MAO inhibition being active for some time ( 5 and 6-APB also have MAO-inhibition)"
no one seems to mention psilocin is not a serotonin releaser
well how come there have been no studies linking psilocin to being cardiotoxic. we all know so well what drugs are cardiotoxic so why cant we say psilocin is cardiotoxic? ECG is not affected by psilocin administration
psilocins efficacy to the receptor is very small
many people take psilocybin . people have been taking it for hundreds of years
we know 5 apb is cardiotoxic for this reason so why would we not know psilocin is cardiotoxic.
mdma has a value of 550 for the receptor but is still cardiotoxic for this reason and suggests there is more to consider than just affinity like the downstream activation profile of psilocin.
do you know what value DMT has? on wiki it says its .108 but on the PDSp database it says its 550
Antagonists in general tend to upregulate receptors, not downregulate them. Yohimbine potentially may be selective for 5-HT2B over 5-HT2A, but yohimbine is not a selective 5-HT2B ligand and has high affinity for alpha2-adrenergic sites.could one take yohimbine before taking psilocin to downregulate the receptor. yohimbine is quite selective for 5ht2b comapred to 2a and 2c so shouldnt affect the experience too much
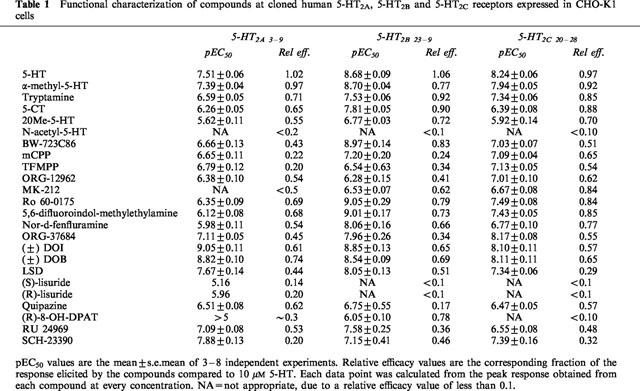
http://www.ouramazingworld.org/uploads/4/3/8/6/43860587/rickli2016.pdf in this study the activation efficacy was so low they could not get a value for it. it had the lowest efficacy for all the tryptamines and less than LSD aswell. how do you know the efficacy of ergotamines and psilocin are the same?
just based of me i know a lot of people who take psilocybin alot. a lot of them dose 2 times a week easily and i even know microdosers. know one i know or on the internet community has ever had a problem. i lot of the patients taking the drugs could detect the issues. they reported a shortness of breathe and a few other things. if you say this to a doctor they will do a few basic things like ECGs and echocardiograms etc there have been no reports ever of a messed up heart structure in the history of psilocybin intake. even if people dont take it as much as the drugs surely if it was a serious risk there would be at least one report but no never has there been one.
It may be difficult to ingest enough yohimbine to block 5-HT2B. Yohimbine tends to produce unpleasant effects due to alpha-2 blockade, which limits the dose people would be able or willing to ingest.does it not take time for it to upregulate the receptor? would yohimbine not block 5ht2b receptors and not allow the receptor to be stimulated from the intake of psilocin. you would have to take the psilocin straight after taking the yohimbine.
You probably won't find any, although they could be made. The structure of the 5-HT2A and 5-HT2B receptors are very similar, so they have very similar pharmacology, meaning that ligands tend to show effects at both. It takes some work to design drugs that are selective for one over the other, although it is possible.do you know any alternative psychedelics that would not have the risk of 5ht2b agonism or at least reduced 5ht2b agonism risk
LSD is pretty selective for 5ht2a over 5ht2b if im not mistaken (Ki 2.7nM vs 30nM)
That isn't enough of a difference to claim selectivity. To completely eliminate the possibility of interaction, you need at least 100-fold selectivity.LSD is pretty selective for 5ht2a over 5ht2b if im not mistaken (Ki 2.7nM vs 30nM)