Jabberwocky
Frumious Bandersnatch
- Joined
- Nov 3, 1999
- Messages
- 84,998
It's no surprise that almost all finding have a contradictory result with other studies, and when translated to humans usually have unpredictable results.
There are a lot of methods used in animals to know if a drug has abuse potential or not, the most used one is "free self-administration" studies, where the animal has a button which administers a drug everytime it is pressed, if they repeatedly press the button then it has potential for abuse. Then in order to determine if some agent has potential for treamtent of addiction, they test how capable it is to modify the rate or dosage of self-administration.
And heres when the problems start, and I give you an example using buspirone (a drug used to augment SSRI effects) and Chlorpromazine (a strong dopamine antagonist)
Heres how much more % of cocaine monkeys self-adminitered when Buspirone was given.

As buspirone dosage increased, the monkeys also increased the number of times they wanted to do cocaine, until a large enough dose, where they stop using cocaine.
and heres the chart for Chlorpromazine
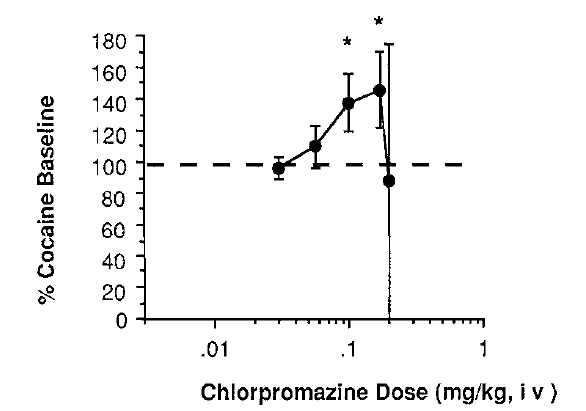
As Chlorpromazine increased, the more cocaine the monkeys did, until the dosage was large enough and they stop using cocaine.
The authors then concluded that buspirone is an agent that can be used to treat cocaine addiction. The reason given is that the charts are identical.
The problem here is that you can intrepret self-administration studies in two different ways:
1) Increase in drug use, means that the rewarding effect has increased, so the animals do more of the drug.
2) Increase in drug use, means that the rewarding effect of the drug has decreased forcing animals to do more of the drug to achieve the same rewarding effects.
The authors choose the intepretation #2, and the identical nature of the charts.
But by looking at the pharmacodynamics of these two drugs you can better understand what is happening.
Buspirone increases seratonin, dopamine and noradrenaline release at low doses, by blocking or downregulating inhibitory mechanisms that prevent too much of these chemicals to be avaible.
At higher doses, it starts to block dopamine receptors acting like a antipsychotic. So the monkeys are pressing the button more often because the drug feels more potent and have more rewarding effects. Until the dosage of buspirone is so great that it acts as a antipsychotic which then they stop using cocaine because it does nothing for them.
Intepretation #1 is what is probably happening with buspirone (yes buspirone increases cocaine and methamphetamine high).
Chlorpromazine is an antipsychotic which blocks dopamine receptors.
So intepretation #2 is what is most likely to happen with chlorpromazine. It is known in humans that dopamine antagonists decrease the effects of stimulants. So this increase in the usage of cocaine is likely happening because they are not feeling as high as before, until the dosage of chlorpromazine is so high that complety stops the effects of cocaine and they stop using.
Just because we know that chlorpromazine decreases the high of cocaine and the study resulted in a identical chart for buspirone and chlorpromazine, doesn't mean they are doing the same thing.
If you start researching studies on drugs of abuse, you will never get anywhere if you follow the authors conclusions. You need to know the pharmacodynamics of the drug + brain of the animal tested (mice are very different from us), + when and how the drugs are given.
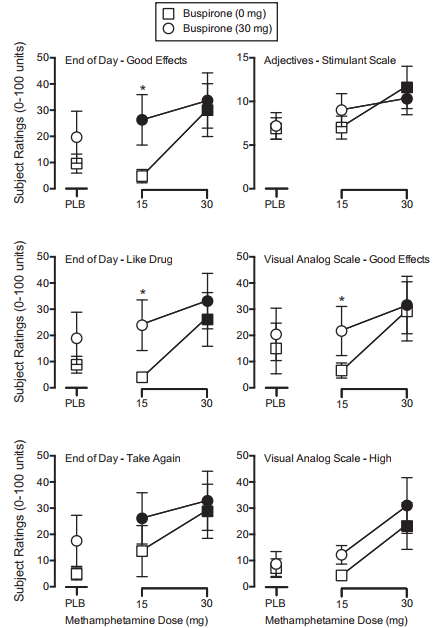
And sure enough, they tested Buspirone in humans and they all reported that their high was higher on buspirone + methamphetamine, than on methamphetamine alone.

This example is just to demonstrate why all studies are flawed, because they all use the same method. You are better off knowing in-vitro pharmacodynamics, in-vivo pharmacokinetics of the drugs and apply some logic.
There are a lot of methods used in animals to know if a drug has abuse potential or not, the most used one is "free self-administration" studies, where the animal has a button which administers a drug everytime it is pressed, if they repeatedly press the button then it has potential for abuse. Then in order to determine if some agent has potential for treamtent of addiction, they test how capable it is to modify the rate or dosage of self-administration.
And heres when the problems start, and I give you an example using buspirone (a drug used to augment SSRI effects) and Chlorpromazine (a strong dopamine antagonist)
Heres how much more % of cocaine monkeys self-adminitered when Buspirone was given.
As buspirone dosage increased, the monkeys also increased the number of times they wanted to do cocaine, until a large enough dose, where they stop using cocaine.
and heres the chart for Chlorpromazine
As Chlorpromazine increased, the more cocaine the monkeys did, until the dosage was large enough and they stop using cocaine.
The authors then concluded that buspirone is an agent that can be used to treat cocaine addiction. The reason given is that the charts are identical.
The problem here is that you can intrepret self-administration studies in two different ways:
1) Increase in drug use, means that the rewarding effect has increased, so the animals do more of the drug.
2) Increase in drug use, means that the rewarding effect of the drug has decreased forcing animals to do more of the drug to achieve the same rewarding effects.
The authors choose the intepretation #2, and the identical nature of the charts.
But by looking at the pharmacodynamics of these two drugs you can better understand what is happening.
Buspirone increases seratonin, dopamine and noradrenaline release at low doses, by blocking or downregulating inhibitory mechanisms that prevent too much of these chemicals to be avaible.
At higher doses, it starts to block dopamine receptors acting like a antipsychotic. So the monkeys are pressing the button more often because the drug feels more potent and have more rewarding effects. Until the dosage of buspirone is so great that it acts as a antipsychotic which then they stop using cocaine because it does nothing for them.
Intepretation #1 is what is probably happening with buspirone (yes buspirone increases cocaine and methamphetamine high).
Chlorpromazine is an antipsychotic which blocks dopamine receptors.
So intepretation #2 is what is most likely to happen with chlorpromazine. It is known in humans that dopamine antagonists decrease the effects of stimulants. So this increase in the usage of cocaine is likely happening because they are not feeling as high as before, until the dosage of chlorpromazine is so high that complety stops the effects of cocaine and they stop using.
Just because we know that chlorpromazine decreases the high of cocaine and the study resulted in a identical chart for buspirone and chlorpromazine, doesn't mean they are doing the same thing.
If you start researching studies on drugs of abuse, you will never get anywhere if you follow the authors conclusions. You need to know the pharmacodynamics of the drug + brain of the animal tested (mice are very different from us), + when and how the drugs are given.
And sure enough, they tested Buspirone in humans and they all reported that their high was higher on buspirone + methamphetamine, than on methamphetamine alone.
This example is just to demonstrate why all studies are flawed, because they all use the same method. You are better off knowing in-vitro pharmacodynamics, in-vivo pharmacokinetics of the drugs and apply some logic.