JohnBoy2000
Bluelighter
- Joined
- May 11, 2016
- Messages
- 2,612
This is the frightening one to me.
I don't have any immediate plans to do it however, given this is done by so many, it's probably worthwhile documenting risks and potential complications.
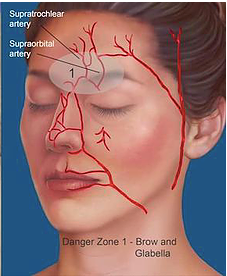
The danger seems to come primarily from the potential to "back-fill" a vessel causing either necrosis, or a vessel that innervates the eye - causing blindness.
Although relatively rare in contrast to how many dermal filler procedures performed, it does happen.
There is recommendation to aspirate before injecting the filler, and always do so slowly to minimize rise - but then I've also read current evidence based research doesn't really support aspirating whilst injecting filler - and in contrast to that again, plenty of recent youtube vids of plastic surgeons strongly advocating aspirating before injecting.
That vid outlays primary danger zones - one being the nasolabial folds, a historically popular area to get filler - but more recently being replaced by cheek filler which stretches the creases indirectly.
I'll add more links as I find them but, harm reduction I guess is the point of focus.
Having spoke with a Dr that performs filler procedures, the area she basically ruled out was glabellar region (between the eyebrows).
I've seen vids of plastic surgeons doing filler here using a cannula, but then they're as expert as one can get.
In contrast to botox, which seems to actually be regarded as one of the safest cosmetic procedures available, that outside possibility of complication with filler no matter how small, well in my case at least would force me to preclude every possible risk before I'd even consider it - understanding no-go areas, risk areas etc.
I don't have any immediate plans to do it however, given this is done by so many, it's probably worthwhile documenting risks and potential complications.
The danger seems to come primarily from the potential to "back-fill" a vessel causing either necrosis, or a vessel that innervates the eye - causing blindness.
Although relatively rare in contrast to how many dermal filler procedures performed, it does happen.
There is recommendation to aspirate before injecting the filler, and always do so slowly to minimize rise - but then I've also read current evidence based research doesn't really support aspirating whilst injecting filler - and in contrast to that again, plenty of recent youtube vids of plastic surgeons strongly advocating aspirating before injecting.
That vid outlays primary danger zones - one being the nasolabial folds, a historically popular area to get filler - but more recently being replaced by cheek filler which stretches the creases indirectly.
I'll add more links as I find them but, harm reduction I guess is the point of focus.
Having spoke with a Dr that performs filler procedures, the area she basically ruled out was glabellar region (between the eyebrows).
I've seen vids of plastic surgeons doing filler here using a cannula, but then they're as expert as one can get.
In contrast to botox, which seems to actually be regarded as one of the safest cosmetic procedures available, that outside possibility of complication with filler no matter how small, well in my case at least would force me to preclude every possible risk before I'd even consider it - understanding no-go areas, risk areas etc.
Last edited: