


Limpet_Chicken
Bluelighter
I'l expand more when I'm not sleep deprived and about to go to bed.
But, I was looking through some stuff, and mirfentanil amongst all the fents jumped out at me, due to in particular its lack of propensity to cause respiratory depression.
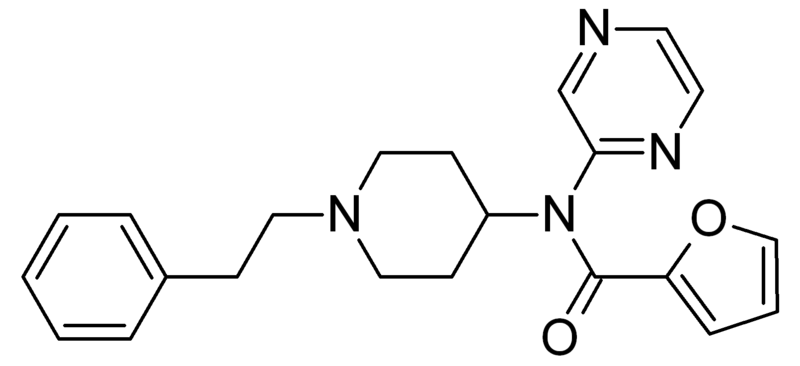
I read a study paper where they infused what for a fentanyl seemed like humongous doses over 30 minutes into volunteers, some of the lucky buggers got upwards of 400mg (not mg/kg, mg total dose)
Also what is the half life/effective duration of activity with mir-fent, has anybody actually tried it, and does anybody know of any similar analogs bearing the pyrazin-2-yl group, or n-furamido moiety on the piperidine ring?
But, I was looking through some stuff, and mirfentanil amongst all the fents jumped out at me, due to in particular its lack of propensity to cause respiratory depression.
I read a study paper where they infused what for a fentanyl seemed like humongous doses over 30 minutes into volunteers, some of the lucky buggers got upwards of 400mg (not mg/kg, mg total dose)
Also what is the half life/effective duration of activity with mir-fent, has anybody actually tried it, and does anybody know of any similar analogs bearing the pyrazin-2-yl group, or n-furamido moiety on the piperidine ring?

