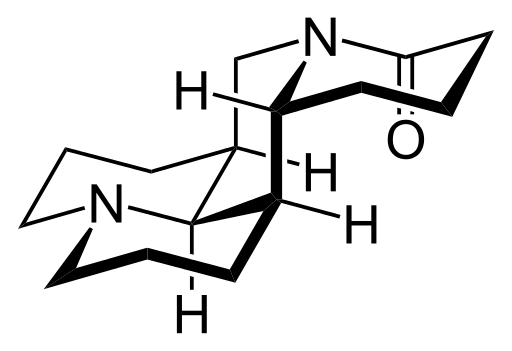
I recently came across a strange website selling this compound, a notably long Kappa-Opioid agonist.
In an effort to collect the truest oddities of the hallucinogenic world, I did some research and found out almost exactly 0 about this drug. There are a few archived threads here on BL but I wanted to bring a new one to life to see if any information has been gathered since freaking 2008.
I can't even get accurate dosing information on it. No half-life; nothing. So, do any of you know anything? Have any of you intrepid souls tried this alien compound?