So I'm heavily considering going back to bupe from heroin/fent but every single time I've gone through monstrous precip WDs. Well, except for the last time and that's what my question is about.
Maybe eighteen or so months ago, I decided to switch to bupe for the fourth, or fifth, or fiftieth time. This time, however, I was gonna wait until I was so sick I wanted to bash my head in before taking anything at all.
So I did. I waited close to 72 hours from the last bit of h and I was sweating, shaking uncontrollably, nearly shit my pants twice, had RLS so bad I spent half the time standing until I collapsed from weakness, and so on.
I took 1mg to start slow like I had read and this time, it seemed to really work! Within 10 minutes, my entire body relaxed and I felt a warm, peaceful sensation. So much so that I fell right asleep.
Two hours later I wake up and the WD symptoms are coming back fast. I told myself, okay, you just probably didn't take enough. So I took another 0.5mg, but this time no noticeable change at all. In fact, it got worse. I was completely confused, annoyed, and angry as hell.
It didn't make sense at the time. Anyways, I end up taking more 0.5mg pieces over the next 36 or so hours and finally the worst was gone (except for the ever present burning sensation in the back of my neck). I wrote it off as another reason I despise bupe and went on with my life.
Four or five months later, however, I ran across an old box of subs that still had all the directions in them. I had never actually read what the drugmaker said because what do they know right? They just synthesize the thing, spend many millions on trials, and stake their reputation on it. Well, according to them, I had been doing it wrong. I had taken the advice of some people on a bupe forum who said to only go up by tiny increments. What the drugmaker said was, and I'm paraphrasing, "Take 2mg. If withdrawal symptoms return within a few hours, take another 2mg or as much more is as needed until you no longer are experiencing any withdrawal symptoms."
All of a sudden, the feeling I got from that first 1mg made sense, and just like the instructions said, my symptoms did return after a few hours. What I DID NOT do was take another 1mg or 2mg. I took 0.25 or 0.5mg doses. It became apparent that what went wrong was that I hadn't taken enough, and therefore suffered for a day and a half until enough microdoses built up on my bloodstream to have an effect.
I had read on forums that taking too much would surely make everything ten times worse. Well, I was an idiot and if I had taken 2mg when I woke back up, Im pretty sure I would've saved myself a great deal of hassle.
So, does this experience ring any bells with anyone else or am I just completely crazy? In retrospect, the symptoms we're getting worse after the microdose because I was in the midst of actual withdrawal and was not taking enough bupe to control it.
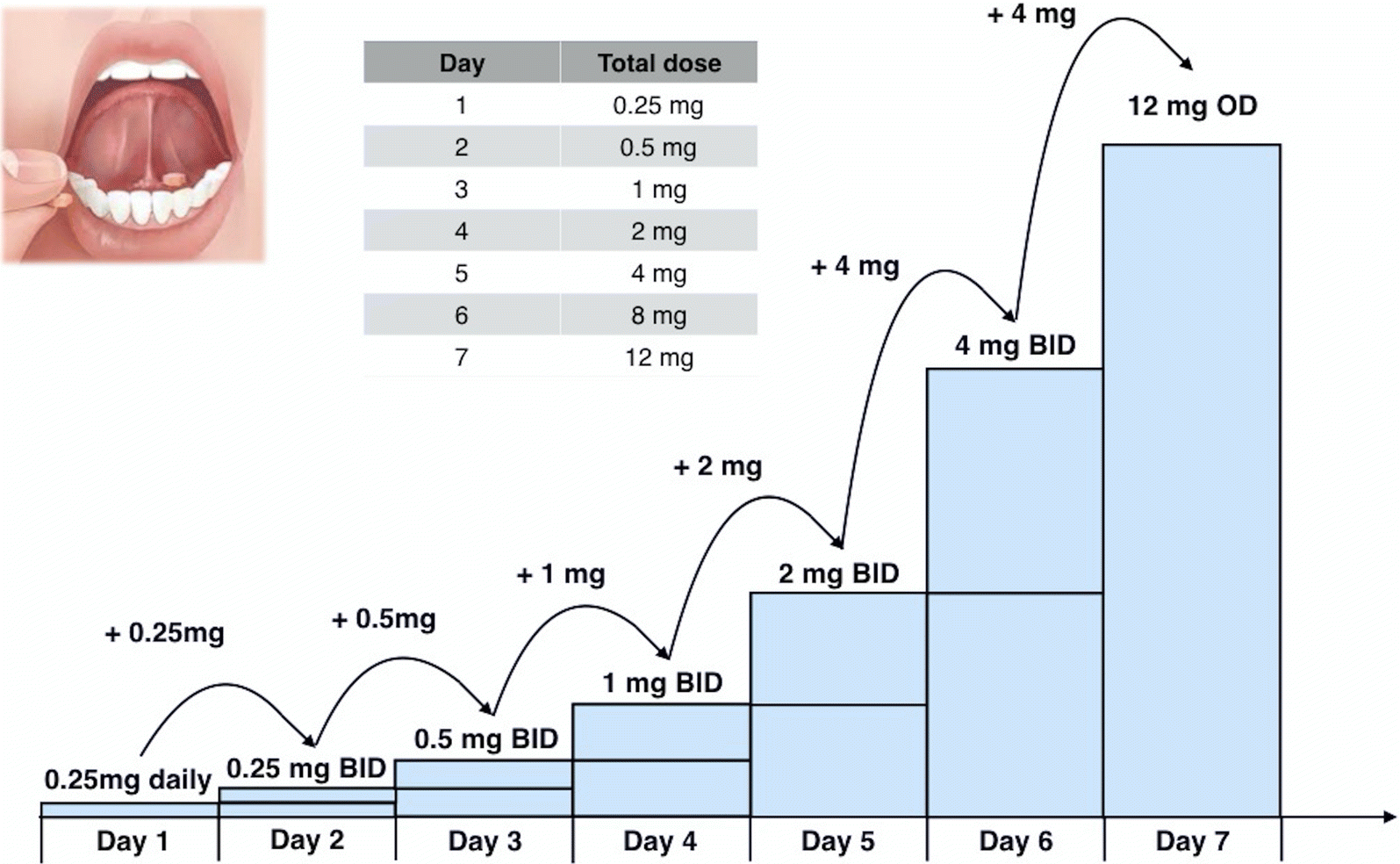
I repeat this story because once again, not by choice, I will be making the move back to bupe once again. I now know about the Bernese method and that sounds promising, but Im also not going to keep microdosing like I did the last time.
Thoughts? Criticisms? Open mockery? Just anyone who can corroborate what I went through will do me a world of good. Thank you.
Maybe eighteen or so months ago, I decided to switch to bupe for the fourth, or fifth, or fiftieth time. This time, however, I was gonna wait until I was so sick I wanted to bash my head in before taking anything at all.
So I did. I waited close to 72 hours from the last bit of h and I was sweating, shaking uncontrollably, nearly shit my pants twice, had RLS so bad I spent half the time standing until I collapsed from weakness, and so on.
I took 1mg to start slow like I had read and this time, it seemed to really work! Within 10 minutes, my entire body relaxed and I felt a warm, peaceful sensation. So much so that I fell right asleep.
Two hours later I wake up and the WD symptoms are coming back fast. I told myself, okay, you just probably didn't take enough. So I took another 0.5mg, but this time no noticeable change at all. In fact, it got worse. I was completely confused, annoyed, and angry as hell.
It didn't make sense at the time. Anyways, I end up taking more 0.5mg pieces over the next 36 or so hours and finally the worst was gone (except for the ever present burning sensation in the back of my neck). I wrote it off as another reason I despise bupe and went on with my life.
Four or five months later, however, I ran across an old box of subs that still had all the directions in them. I had never actually read what the drugmaker said because what do they know right? They just synthesize the thing, spend many millions on trials, and stake their reputation on it. Well, according to them, I had been doing it wrong. I had taken the advice of some people on a bupe forum who said to only go up by tiny increments. What the drugmaker said was, and I'm paraphrasing, "Take 2mg. If withdrawal symptoms return within a few hours, take another 2mg or as much more is as needed until you no longer are experiencing any withdrawal symptoms."
All of a sudden, the feeling I got from that first 1mg made sense, and just like the instructions said, my symptoms did return after a few hours. What I DID NOT do was take another 1mg or 2mg. I took 0.25 or 0.5mg doses. It became apparent that what went wrong was that I hadn't taken enough, and therefore suffered for a day and a half until enough microdoses built up on my bloodstream to have an effect.
I had read on forums that taking too much would surely make everything ten times worse. Well, I was an idiot and if I had taken 2mg when I woke back up, Im pretty sure I would've saved myself a great deal of hassle.
So, does this experience ring any bells with anyone else or am I just completely crazy? In retrospect, the symptoms we're getting worse after the microdose because I was in the midst of actual withdrawal and was not taking enough bupe to control it.
I repeat this story because once again, not by choice, I will be making the move back to bupe once again. I now know about the Bernese method and that sounds promising, but Im also not going to keep microdosing like I did the last time.
Thoughts? Criticisms? Open mockery? Just anyone who can corroborate what I went through will do me a world of good. Thank you.
")