This is the presentation I presented on Wednesday at this conference. I'm interested to hear any feedback or just thoughts from you. I will be putting together some academic papers on the issue over the next few months. (sorry the pics are so big!!)
GHB use and harms in Melbourne
In the first half of this talk, I will discuss trends in GHB use and harms; then run through the findings from two data sources drawn from Melbourne populations – GHB cases attended by ambulance, and regular ecstasy users who also use GHB. I’ve selected some of the more interesting findings to talk through in detail for the latter half of the presentation, including market comparisons of GHB with ecstasy and speed, and settings of GHB use versus settings of overdose. Finally, I will present the limitations of the data, a summary of key findings, and some unanswered questions.
So, what is GHB? GHB, or Gamma-hydroxybutyrate, is known in Melbourne simply as ‘G’. Other less common names include fantasy, liquid ecstasy, & GBH. GHB is a depressant drug used recreationally for its euphoric, sedative and aphrodisiac qualities. In Australia, it is almost always consumed as a liquid.
GHB has been associated with the nightclub and rave scene, body-building, and drink-spiking, as well as being used to treat narcolepsy, and alcohol and opiate dependence.
With GHB, there is a fine line between an effective recreational dose and an overdose, which is characterised by loss of consciousness and respiratory depression. Overdose can result in seizure, coma and in some cases, death. Heavy daily users of GHB have been known to experience dependence and withdrawal.
GHB was made illegal in Victoria in 1997, and this lead users towards GHB analogues such as gamma-butyrolactone (GBL) and 1,4-butanediol (1,4-B), which are converted to GHB after ingestion. Although pharmacologically different from GHB, these precursors pose similar or greater risks.
Both chemicals have legitimate industrial uses, so federal law now requires the buyer to sign an End User Declaration stating what the chemicals will be used for.
According to some ecstasy users and the tabloid press, the GHB sold in Melbourne is actually 1,4-B. Apparently 1,4-B is more commonly available in Melbourne, and 1,4-B users mistakenly believe they are using GHB. This ecstasy user stated that what is known as ‘G’ is really 1,4-B.
This understanding was echoed in tabloid media. The first sentence of this newspaper article states that many of those who think they are using GHB are actually swallowing chemicals used to make nail varnish remover.
So, what do we know about trends in GHB use and harms?
In the UK and USA, GHB is rarely included drug trends surveys. In Australia, the most recent National Drug Strategy Household Survey was the first to include questions specific to GHB, finding only a very small number of people had used it. Data from the national Party Drug Initiative showed that 10% of regular ecstasy users reported GHB use in the preceding 6 months. This use was concentrated in Melbourne and Sydney.
Only two studies of GHB users were found in the literature review. Both samples were mostly male, employed, and had an average age of 26 to 27. Most of the California sample used GHB weekly or more often, whereas the Sydney sample used GHB less than once a month on average. The majority of both samples said they had lost consciousness on GHB at least once.
In Melbourne, GHB overdoses have recently attracted heavy media attention. The 2004 PDI showed recent use of GHB and 1,4-B was highest in Melbourne compared to all other capital cities. However beyond this, we found a lack of information on GHB use and harms in Melbourne. We examined the datasets available to us, and found only two could provide more information about GHB. These were: the ambulance attendance database and the ecstasy user data from the Party drug Initiative. I’ll present summaries of what we found from both datasets, then take a closer look at a few areas of interest.
Turning Point, in collaboration with the Victorian Metropolitan Ambulance Service, maintains an electronic database of ambulance attendances where drug use or overdose is indicated. The data I will present today is from the period March 2001 – September 2003.
Ambulance attendances involving GHB were relatively rare compared to those involving other drugs, especially alcohol and heroin.
Where additional drugs are reported in GHB cases, these tend to be ecstasy, alcohol and amphetamine. Polydrug use was indicated in more than half of the GHB cases.
The rest of the analysis compared characteristics of GHB cases with those of ecstasy, amphetamine and heroin cases.
The Australian Party Drug Initiative (PDI) is an annual survey of trends in drug use and drug markets among regular users of ecstasy. Data on use of GHB and its analogues are collected.
Here are some definitions for the terms I’ll use:
In the following analyses, data for GHB and 1,4-B users has been combined. We decided to do this because GHB and 1,4-B users are probably using the same drug, but there appear to be differences in knowledge about the drug’s chemical content. There were 34 recent GHB/1,4-B users in 2004. The following findings relate to 2004 Melbourne data unless stated.
Recent GHB/1,4-B users were mostly employed or studying. Half the sample used GHB/1,4-B regularly. Regular users were younger and less likely to be male, than the other half of the sample, who used GHB/1,4-B occasionally. Almost half of the regular users used GHB/1,4-B weekly or more often.
All were polydrug users, but this is the nature of the sample, who were recruited based on their use of ecstasy.
GHB/1,4-B was reported as much cheaper than ecstasy and methamphetamines, and all were easily obtained.
GHB/1,4-B was usually used in both public and private settings, as were ecstasy and methamphetamines. Public settings (eg. nightclubs) were most popular for ecstasy and methamphetamine use, whereas a friend’s home was the most often mentioned setting of GHB/1,4-B use.
38% of GHB/1,4-B users stated they had overdosed in the last 6 months, with more frequent users more likely to report a recent overdose. Overdose was defined as ‘passed out or fallen into a coma’.
Almost all reported concurrent use of other drugs at the time of overdose.
Only 2 accessed health and medical services, including ambulance, first aid, and emergency dept, however no-one was admitted to hospital.
Awareness of overdose symptoms and risks was high among the 2003 sample when this question was asked. Recent GHB/1,4-B users were able to name risks which focused on overdose symptoms, the danger of mixing with alcohol, and unknown purity making it difficult to measure the right dose.
So now I’ve finished the summary of findings from both datasets. I’ve put this slide in to break things up a bit.

On the left is one of the posters from the Victorian government’s “GHB is never safe” campaign.
On the right are some images from the ‘Say no to G’ industry-lead campaign. Badges like the one shown, were distributed and worn, and others (like the raver pictured) went to a lot of trouble getting their message across.
The message from both campaigns is one of zero tolerance to GHB and GHB users.
Now I’ll run through two areas in more detail:
market comparisons, and
settings of use versus settings of overdose.
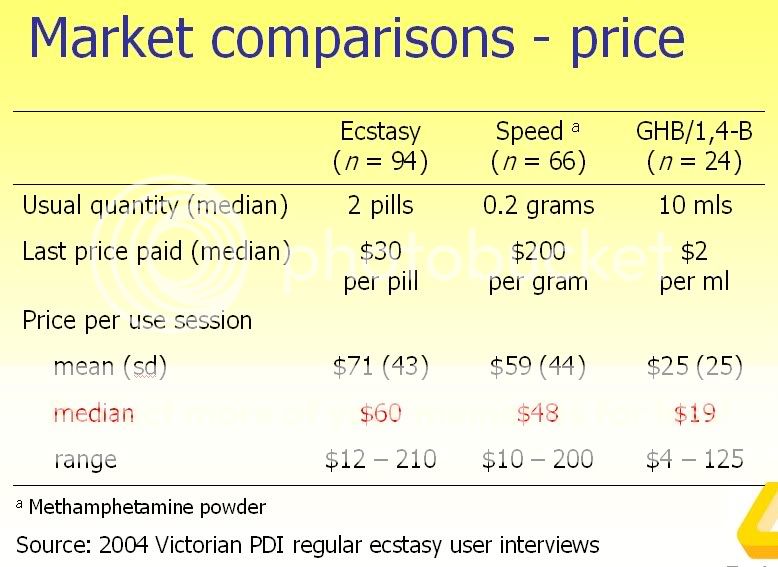
This table compares prices for GHB/1,4-B with ecstasy and methamphetamine powder or speed.
To enable a fair price comparison, we calculated how much it would cost for one session of use with each drug. This was done by multiplying the usual quantity reportedly used by the last price paid by that person, once both values were converted into the same measure. In the case of speed, all weighted measures were converted to grams using the conversion of 1 point equalling .1 of a gram.
Using these methods, the price of a session of ecstasy use was three times the price of a session of GHB or 1,4-B use. A session of speed use was more than twice the price.
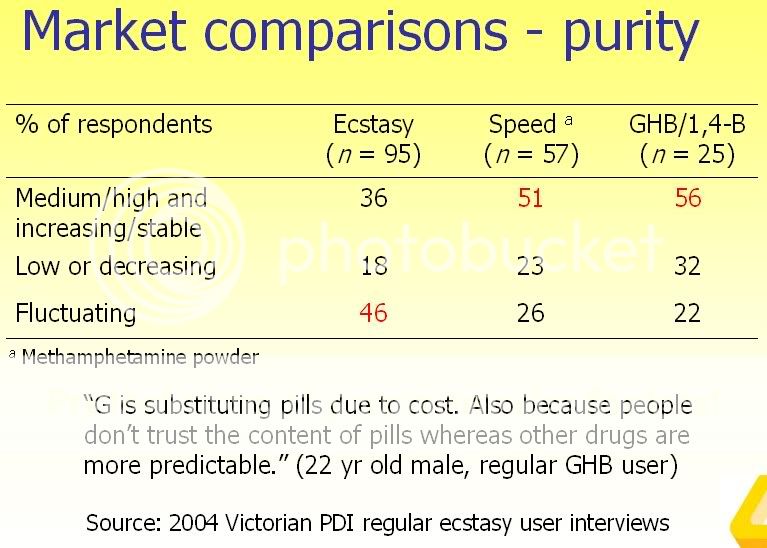
This slide compares the perceived purity of ecstasy, speed and GHB/1,4-B.
Participants who felt confident enough to talk about the market for each drug were asked whether the current strength or purity was low, medium, high or fluctuating. Then they were asked whether the purity had been increasing, stable, decreasing or fluctuating over the last 6 months.
Medium to high and increasing or stable purity represents the ideal situation from the drug users point of view, as opposed to low, decreasing or fluctuating purity. Looking at the numbers in red, you can see that the purity of ecstasy was more likely to be perceived as fluctuating than speed or GHB.
The quote from this regular GHB user summarises the situation well: He states that GHB is taking the place of ecstasy due to cost and differences in perceived purity.
It was mentioned previously that most ambulances who attended GHB cases were called to public settings, and that GHB and 1,4-B users report using these drugs in both public and private settings. This slide compares these data directly.
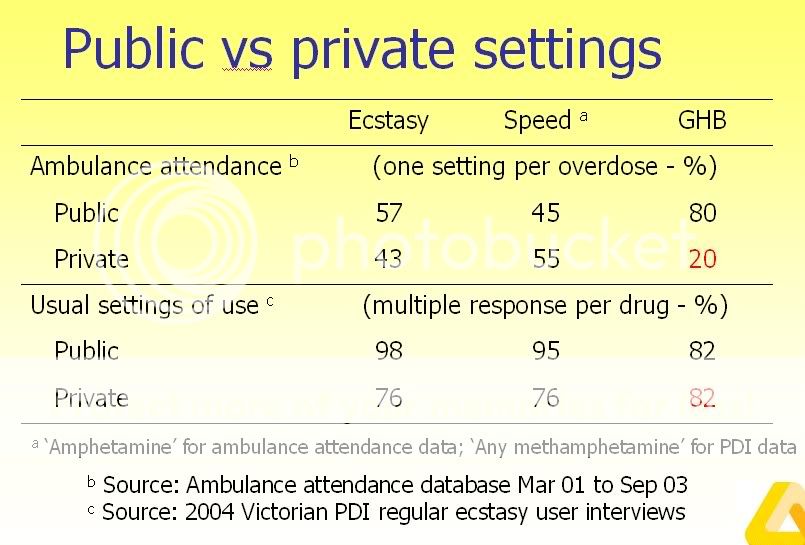
Given that most users reported use in public and private settings, all things being equal, we would expect ambulances to be called to both settings. We see this pattern for ecstasy and speed, but not for GHB. Although GHB is used in private homes, ambulances are rarely called to these locations.
Why is this the case?
One explanation is that GHB users are overdosing in private settings, and are less likely to be assisted, perhaps due to the absence of nightclub staff with explicit instruction to act in the case of overdose.
Another possibility is that GHB use in private settings may be somehow less likely to result in overdose. For example, dosage measurement may be more accurate in a home environment compared to a nightclub. Additionally, the nightclub context may be more conducive to excessive use than the private context.
Given that the GHB user data was obtained using a small convenience sample, errors in sampling may be the reason for this anomaly.
Replication and further in-depth research are needed.
This research has a number of limitations. We were limited to analysing only two datasets because no other data sources available to us coded specifically for GHB. The datasets we did use were not designed specifically to capture information on GHB or 1,-4B, which meant that certain items of particular interest were not recorded. Our data from the PDI were based on a small convenience sample. These characteristics of the sample limit the confidence we can have that our findings represent what is actually happening. Finally, our data sources lacked qualitative and/or contextual data, which would have helped to interpret contradictory findings. The qualitative inquiry into GHB use in Melbourne recently conducted by Cameron Duff, formerly from the Australian Drug Foundation, will be most useful to combine with the findings reported here.
In summary, we have conducted an exploratory analysis on GHB use and harms in Melbourne.
We found that:
GHB overdose was common among GHB users, who used the drug despite being well aware of this risk. Only 15% received medical attention for their overdose.
Some market characteristics of GHB, such as its considerably lower price and apparently less variable purity, have lead to some groups using GHB in place of ecstasy.
Although GHB was used in both public and private settings, ambulances mostly attended GHB overdoses in public settings.
Finally, I’ll leave you to ponder some unanswered questions.
What are the characteristics of GHB overdoses where an ambulance is not called?
What is safer or more dangerous about private versus public settings in terms of GHB related harms?
How effective were the government and peer led anti-G campaigns? Were there any unintended consequences?
For example, if the message 'Go Home G heads' was taken literally, private settings may be a very important place to focus efforts to prevent GHB related harms.
Thanks!
Acknowledgements
drug users who participated and advised
Vic Dept of Human Services
Aust Govt Dept of Health & Ageing
Vic Metropolitan Ambulance Service
National Drug & Alcohol Research Centre
Mark Stoové, Stefan Cvetkovski, Belinda Grant, Justine Spicer, Robyn Dwyer, Paul McElwee
Email me at [email protected]
GHB use and harms in Melbourne
In the first half of this talk, I will discuss trends in GHB use and harms; then run through the findings from two data sources drawn from Melbourne populations – GHB cases attended by ambulance, and regular ecstasy users who also use GHB. I’ve selected some of the more interesting findings to talk through in detail for the latter half of the presentation, including market comparisons of GHB with ecstasy and speed, and settings of GHB use versus settings of overdose. Finally, I will present the limitations of the data, a summary of key findings, and some unanswered questions.
So, what is GHB? GHB, or Gamma-hydroxybutyrate, is known in Melbourne simply as ‘G’. Other less common names include fantasy, liquid ecstasy, & GBH. GHB is a depressant drug used recreationally for its euphoric, sedative and aphrodisiac qualities. In Australia, it is almost always consumed as a liquid.
GHB has been associated with the nightclub and rave scene, body-building, and drink-spiking, as well as being used to treat narcolepsy, and alcohol and opiate dependence.
With GHB, there is a fine line between an effective recreational dose and an overdose, which is characterised by loss of consciousness and respiratory depression. Overdose can result in seizure, coma and in some cases, death. Heavy daily users of GHB have been known to experience dependence and withdrawal.
GHB was made illegal in Victoria in 1997, and this lead users towards GHB analogues such as gamma-butyrolactone (GBL) and 1,4-butanediol (1,4-B), which are converted to GHB after ingestion. Although pharmacologically different from GHB, these precursors pose similar or greater risks.
Both chemicals have legitimate industrial uses, so federal law now requires the buyer to sign an End User Declaration stating what the chemicals will be used for.
According to some ecstasy users and the tabloid press, the GHB sold in Melbourne is actually 1,4-B. Apparently 1,4-B is more commonly available in Melbourne, and 1,4-B users mistakenly believe they are using GHB. This ecstasy user stated that what is known as ‘G’ is really 1,4-B.
This understanding was echoed in tabloid media. The first sentence of this newspaper article states that many of those who think they are using GHB are actually swallowing chemicals used to make nail varnish remover.
So, what do we know about trends in GHB use and harms?
In the UK and USA, GHB is rarely included drug trends surveys. In Australia, the most recent National Drug Strategy Household Survey was the first to include questions specific to GHB, finding only a very small number of people had used it. Data from the national Party Drug Initiative showed that 10% of regular ecstasy users reported GHB use in the preceding 6 months. This use was concentrated in Melbourne and Sydney.
Only two studies of GHB users were found in the literature review. Both samples were mostly male, employed, and had an average age of 26 to 27. Most of the California sample used GHB weekly or more often, whereas the Sydney sample used GHB less than once a month on average. The majority of both samples said they had lost consciousness on GHB at least once.
In Melbourne, GHB overdoses have recently attracted heavy media attention. The 2004 PDI showed recent use of GHB and 1,4-B was highest in Melbourne compared to all other capital cities. However beyond this, we found a lack of information on GHB use and harms in Melbourne. We examined the datasets available to us, and found only two could provide more information about GHB. These were: the ambulance attendance database and the ecstasy user data from the Party drug Initiative. I’ll present summaries of what we found from both datasets, then take a closer look at a few areas of interest.
Turning Point, in collaboration with the Victorian Metropolitan Ambulance Service, maintains an electronic database of ambulance attendances where drug use or overdose is indicated. The data I will present today is from the period March 2001 – September 2003.
Ambulance attendances involving GHB were relatively rare compared to those involving other drugs, especially alcohol and heroin.
Where additional drugs are reported in GHB cases, these tend to be ecstasy, alcohol and amphetamine. Polydrug use was indicated in more than half of the GHB cases.
The rest of the analysis compared characteristics of GHB cases with those of ecstasy, amphetamine and heroin cases.
- GHB overdose cases had a mean age of 25 years and were two-thirds male. GHB and ecstasy cases were significantly younger than heroin and amphetamine cases.
- Breath rate and consciousness were significantly lower in GHB cases than for the stimulant drug overdoses. GHB overdoses were similar to heroin in terms of clinical presentation.
- GHB cases almost always occurred on the weekend, and between midnight and midday. This pattern was similar to ecstasy cases, but quite different from heroin and amphetamine cases.
- 80% of GHB cases were attended in public places. The figure was significantly higher than heroin, ecstasy or amphetamine cases.
- 92% of GHB cases were transported to hospital, compared to about three quarters of ecstasy and amphetamine cases, and only 22% of heroin cases.
The Australian Party Drug Initiative (PDI) is an annual survey of trends in drug use and drug markets among regular users of ecstasy. Data on use of GHB and its analogues are collected.
Here are some definitions for the terms I’ll use:
- recent use is at least once in last 6 months
- occasional use is less than monthly use
- regular use is monthly or more often
In the following analyses, data for GHB and 1,4-B users has been combined. We decided to do this because GHB and 1,4-B users are probably using the same drug, but there appear to be differences in knowledge about the drug’s chemical content. There were 34 recent GHB/1,4-B users in 2004. The following findings relate to 2004 Melbourne data unless stated.
Recent GHB/1,4-B users were mostly employed or studying. Half the sample used GHB/1,4-B regularly. Regular users were younger and less likely to be male, than the other half of the sample, who used GHB/1,4-B occasionally. Almost half of the regular users used GHB/1,4-B weekly or more often.
All were polydrug users, but this is the nature of the sample, who were recruited based on their use of ecstasy.
GHB/1,4-B was reported as much cheaper than ecstasy and methamphetamines, and all were easily obtained.
GHB/1,4-B was usually used in both public and private settings, as were ecstasy and methamphetamines. Public settings (eg. nightclubs) were most popular for ecstasy and methamphetamine use, whereas a friend’s home was the most often mentioned setting of GHB/1,4-B use.
38% of GHB/1,4-B users stated they had overdosed in the last 6 months, with more frequent users more likely to report a recent overdose. Overdose was defined as ‘passed out or fallen into a coma’.
Almost all reported concurrent use of other drugs at the time of overdose.
Only 2 accessed health and medical services, including ambulance, first aid, and emergency dept, however no-one was admitted to hospital.
Awareness of overdose symptoms and risks was high among the 2003 sample when this question was asked. Recent GHB/1,4-B users were able to name risks which focused on overdose symptoms, the danger of mixing with alcohol, and unknown purity making it difficult to measure the right dose.
So now I’ve finished the summary of findings from both datasets. I’ve put this slide in to break things up a bit.
On the left is one of the posters from the Victorian government’s “GHB is never safe” campaign.
On the right are some images from the ‘Say no to G’ industry-lead campaign. Badges like the one shown, were distributed and worn, and others (like the raver pictured) went to a lot of trouble getting their message across.
The message from both campaigns is one of zero tolerance to GHB and GHB users.
Now I’ll run through two areas in more detail:
market comparisons, and
settings of use versus settings of overdose.
This table compares prices for GHB/1,4-B with ecstasy and methamphetamine powder or speed.
To enable a fair price comparison, we calculated how much it would cost for one session of use with each drug. This was done by multiplying the usual quantity reportedly used by the last price paid by that person, once both values were converted into the same measure. In the case of speed, all weighted measures were converted to grams using the conversion of 1 point equalling .1 of a gram.
Using these methods, the price of a session of ecstasy use was three times the price of a session of GHB or 1,4-B use. A session of speed use was more than twice the price.
This slide compares the perceived purity of ecstasy, speed and GHB/1,4-B.
Participants who felt confident enough to talk about the market for each drug were asked whether the current strength or purity was low, medium, high or fluctuating. Then they were asked whether the purity had been increasing, stable, decreasing or fluctuating over the last 6 months.
Medium to high and increasing or stable purity represents the ideal situation from the drug users point of view, as opposed to low, decreasing or fluctuating purity. Looking at the numbers in red, you can see that the purity of ecstasy was more likely to be perceived as fluctuating than speed or GHB.
The quote from this regular GHB user summarises the situation well: He states that GHB is taking the place of ecstasy due to cost and differences in perceived purity.
It was mentioned previously that most ambulances who attended GHB cases were called to public settings, and that GHB and 1,4-B users report using these drugs in both public and private settings. This slide compares these data directly.
Given that most users reported use in public and private settings, all things being equal, we would expect ambulances to be called to both settings. We see this pattern for ecstasy and speed, but not for GHB. Although GHB is used in private homes, ambulances are rarely called to these locations.
Why is this the case?
One explanation is that GHB users are overdosing in private settings, and are less likely to be assisted, perhaps due to the absence of nightclub staff with explicit instruction to act in the case of overdose.
Another possibility is that GHB use in private settings may be somehow less likely to result in overdose. For example, dosage measurement may be more accurate in a home environment compared to a nightclub. Additionally, the nightclub context may be more conducive to excessive use than the private context.
Given that the GHB user data was obtained using a small convenience sample, errors in sampling may be the reason for this anomaly.
Replication and further in-depth research are needed.
This research has a number of limitations. We were limited to analysing only two datasets because no other data sources available to us coded specifically for GHB. The datasets we did use were not designed specifically to capture information on GHB or 1,-4B, which meant that certain items of particular interest were not recorded. Our data from the PDI were based on a small convenience sample. These characteristics of the sample limit the confidence we can have that our findings represent what is actually happening. Finally, our data sources lacked qualitative and/or contextual data, which would have helped to interpret contradictory findings. The qualitative inquiry into GHB use in Melbourne recently conducted by Cameron Duff, formerly from the Australian Drug Foundation, will be most useful to combine with the findings reported here.
In summary, we have conducted an exploratory analysis on GHB use and harms in Melbourne.
We found that:
GHB overdose was common among GHB users, who used the drug despite being well aware of this risk. Only 15% received medical attention for their overdose.
Some market characteristics of GHB, such as its considerably lower price and apparently less variable purity, have lead to some groups using GHB in place of ecstasy.
Although GHB was used in both public and private settings, ambulances mostly attended GHB overdoses in public settings.
Finally, I’ll leave you to ponder some unanswered questions.
What are the characteristics of GHB overdoses where an ambulance is not called?
What is safer or more dangerous about private versus public settings in terms of GHB related harms?
How effective were the government and peer led anti-G campaigns? Were there any unintended consequences?
For example, if the message 'Go Home G heads' was taken literally, private settings may be a very important place to focus efforts to prevent GHB related harms.
Thanks!
Acknowledgements
drug users who participated and advised
Vic Dept of Human Services
Aust Govt Dept of Health & Ageing
Vic Metropolitan Ambulance Service
National Drug & Alcohol Research Centre
Mark Stoové, Stefan Cvetkovski, Belinda Grant, Justine Spicer, Robyn Dwyer, Paul McElwee
Email me at [email protected]
")