-
N&PD Moderators: Skorpio | thegreenhand
-
Neuroscience & Pharmacology Discussion Welcome Guest
Posting Rules Bluelight Rules Recent Journal Articles Chemistry Mega-Thread FREE Chemistry Databases! Self-Education Guide
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Are there any good SNDRIs yet?
- Thread starter atara
- Start date
atara
Bluelighter
- Joined
- Apr 1, 2010
- Messages
- 2,785
I suppose I had forgotten that MAO-B inhibitors aren't really serotonergic. Selegiline/rasagiline thus count. Interestingly p-benzyloxyamphetamine is a reversible (kinda) selective MAO-B inhibitor, cf https://www.sciencedirect.com/science/article/pii/S0968089609001333 (Table 2, entry 3f).
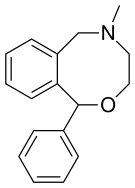
Nefopam is an SNRI and 5-ht2c antagonist, so it resembles both SNRIs and agomelatine.
Nefopam is an SNRI and 5-ht2c antagonist, so it resembles both SNRIs and agomelatine.
polymath
Bluelight Crew
- Joined
- Nov 4, 2010
- Messages
- 1,884
Here's a reference for DAT binding of orphenadrine.

 www.ncbi.nlm.nih.gov
www.ncbi.nlm.nih.gov
And here's a ref about a FAAH enzyme deletion mutation that causes insensitivity to pain and anxiety, without making one unable to avoid hurting themself (someone mentioned people having something like this because of NaV1.7 deletion, which is a different thing):

 www.sciencedirect.com
www.sciencedirect.com
Insights into the Modulation of Dopamine Transporter Function by Amphetamine, Orphenadrine, and Cocaine Binding
Human dopamine (DA) transporter (hDAT) regulates dopaminergic signaling in the central nervous system by maintaining the synaptic concentration of DA at physiological levels, upon reuptake of DA into presynaptic terminals. DA translocation involves the ...
www.ncbi.nlm.nih.gov
And here's a ref about a FAAH enzyme deletion mutation that causes insensitivity to pain and anxiety, without making one unable to avoid hurting themself (someone mentioned people having something like this because of NaV1.7 deletion, which is a different thing):
Microdeletion in a FAAH pseudogene identified in a patient with high anandamide concentrations and pain insensitivity
The study of rare families with inherited pain insensitivity can identify new human-validated analgesic drug targets. Here, a 66-yr-old female present…
Last edited:
sekio
Bluelight Crew
- Joined
- Sep 14, 2009
- Messages
- 21,994
I always thought nefopam was kind of cool. Take diphenhydramine, an antihistamine, and wrap its 'tail' around to cyclize it and ... wham! A non-opioid painkiller that is also a SNDRI.
Also, insensitivity to anxiety? Some people would give their first-born child for that. Hell, I'd give my left leg, and then I wouldn't worry about it because I wouldn't be anxious over losing a leg!
If it does, I never noticed them, and believe me I've taken my fair share of naproxen. The better part of two years was filled with 2x220mg naproxen sodium, 3 times a day, every day, That's 1.32g naproxen sodium a day, or almost 500 grams a year. If there were psychoactive effects they were very subtle. To the best of my knowledge nobody even abuses the shit in prisons where they'll snort Seroquel or Wellbutrin just to get a rush. (Neither the package insert nor the package (inner or outer) on my Bayer Aleve (Canadian) mention euphoria or any psychic disturbances either.)
Also, insensitivity to anxiety? Some people would give their first-born child for that. Hell, I'd give my left leg, and then I wouldn't worry about it because I wouldn't be anxious over losing a leg!
Naproxen especially has psychoactive effects
If it does, I never noticed them, and believe me I've taken my fair share of naproxen. The better part of two years was filled with 2x220mg naproxen sodium, 3 times a day, every day, That's 1.32g naproxen sodium a day, or almost 500 grams a year. If there were psychoactive effects they were very subtle. To the best of my knowledge nobody even abuses the shit in prisons where they'll snort Seroquel or Wellbutrin just to get a rush. (Neither the package insert nor the package (inner or outer) on my Bayer Aleve (Canadian) mention euphoria or any psychic disturbances either.)
Last edited:
checktest
Bluelighter
- Joined
- Jun 9, 2013
- Messages
- 338
Yeah, I didn't notice anything on 500mg naproxen bid as well. No euphoria but mood changes was mentioned on the insert. Prefer ketoprofen anyways, though it doesn't last as long.
Also, with FAAH, that was a tricky area after those deaths with that FAAH inhibitor. Looks like they got some of the off-target problems identified though. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5641481/
The trial for reference: https://www.sciencemag.org/news/2017/06/new-clues-why-french-drug-trial-went-horribly-wrong
Also, with FAAH, that was a tricky area after those deaths with that FAAH inhibitor. Looks like they got some of the off-target problems identified though. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5641481/
The trial for reference: https://www.sciencemag.org/news/2017/06/new-clues-why-french-drug-trial-went-horribly-wrong
polymath
Bluelight Crew
- Joined
- Nov 4, 2010
- Messages
- 1,884
Salicylate poisoning can cause ringing in the ears and some other neuro symptoms, but definitely isn't any good as a drug...
The effect of FAAH enzyme missing in the first place could be different from taking a large dose of a FAAH inhibitor.
None of the antihistamines in common use probably is a good enough stimulant to have much effect unless dosed by some fast route by someone who practically never uses stimulants. Trying to counterbalance the side effects with a muscarine agonist would be way too dangerous, especially if someone gets the genius idea of taking it intravenously and has their heart stop when that crap all goes through it at once on first pass. Not sure if the way how orphenadrine blocks the dopamine transporter even is of the type that causes euphoria, some tropane derivatives just have an anti-ADHD and anti-parkinson effect without mood elevation. Haven't seen any 3,4-dichlorinated derivatives of ethylenediamine antihistamines tested for DAT binding, in fact it hasn't been done even for 3,4-dichlorobenzylpiperazine.
The effect of FAAH enzyme missing in the first place could be different from taking a large dose of a FAAH inhibitor.
None of the antihistamines in common use probably is a good enough stimulant to have much effect unless dosed by some fast route by someone who practically never uses stimulants. Trying to counterbalance the side effects with a muscarine agonist would be way too dangerous, especially if someone gets the genius idea of taking it intravenously and has their heart stop when that crap all goes through it at once on first pass. Not sure if the way how orphenadrine blocks the dopamine transporter even is of the type that causes euphoria, some tropane derivatives just have an anti-ADHD and anti-parkinson effect without mood elevation. Haven't seen any 3,4-dichlorinated derivatives of ethylenediamine antihistamines tested for DAT binding, in fact it hasn't been done even for 3,4-dichlorobenzylpiperazine.
- Joined
- Jul 2, 2008
- Messages
- 9,131
I suppose I had forgotten that MAO-B inhibitors aren't really serotonergic. Selegiline/rasagiline thus count. Interestingly p-benzyloxyamphetamine is a reversible (kinda) selective MAO-B inhibitor, cf https://www.sciencedirect.com/science/article/pii/S0968089609001333 (Table 2, entry 3f).
Nefopam is an SNRI and 5-ht2c antagonist, so it resembles both SNRIs and agomelatine.
Not a very educated guess, but at high enough doses, would MAO-B inhibitors work on MAO-A/cactechol-o-methyltransferase at high enough doses. As selegiline wrt MAO-B/MAO-A.
I think ketamine is an SNDRI. And an opioid agonist. Yeesh.
The problem with an SNDRI as an antidepressant is that you're giving it to the population whom are most likely to abuse it.
In honesty, coca farmers in SA get along well with it, but pure cocaine is another beast. As I understand, coca leaf not only offers energy, but is also nutritious and otherwise healthy, not to mention offers a chew and is grown with soil that isn't Monsanto-ized, as the crop has yet to be officially recognized via global approval---thanks a lot, Amurca. In this respect, it is "good", lasting more than 20-30 minutes, and not being cut with chemotherapy drugs.
sekio
Bluelight Crew
- Joined
- Sep 14, 2009
- Messages
- 21,994
I think ketamine is an SNDRI. And an opioid agonist. Yeesh.
It's a dissociative first and foremost. Not a very strong SNDRI or opioid.
ChemicallyEnhanced
Bluelighter
- Joined
- Apr 29, 2018
- Messages
- 9,489
I think I'm really deficient in dopamine and would get ENORMOUS benefit from this type of med. My SSRI had made a huge difference but not enough. Also, I once got a very shady doctor to prescribe me amphetamines for depression (TBF he must have been in his late 70s so this would have been common practice when he was a young doctor). Each pill was 175mg Amphetamine Sulphate and I was prescribed 5 a day (with 180mg Phenobarbital at night to sleep) and it was a fucking miracle cure for my depression. I was always very happy. The only reason I stopped was because I became totally psychotic and was hospitalized for Paranoid Schizophrenia (which was obviously a miss-diagnoses: I had Amphetamine-Induced Psychosis).
Opiates work almost as well, and again, they significantly increase your dopamine.
Opiates work almost as well, and again, they significantly increase your dopamine.
sekio
Bluelight Crew
- Joined
- Sep 14, 2009
- Messages
- 21,994
If you were 'deficient in dopamine' you would present with Parkinsons, not depression.
I somehow doubt you were prescribed 875mg of amphetamine salts a day. If the pharmacist saw a script for that I'd bet they'd laugh you out of the pharmacy. The highest dose of Adderall that is manufactured is a measly 30mg so you'd need to have your monster caps custom-made. If you were taking almost a gram of amphetamine per day, then you'd absolutely need a solid whack of phenobarbital to put you to sleep. I'd also be amazed if you didn't go off the rails and go totally bonkers either. People who take "heroic" doses of amphetamines have this unfortunate tendency to eventually neglect diet and sleep to the point where your mind just implodes into itself and the Shadow People are trying to convince you to kill your family.
Nowadays amphetamine is only rarely if ever prescribed as an antidepressant. It would be more accurate to say that at such high dosages it's more of a recreational euphoriant drug than a true antidepressant. Antidepressants are not supposed to make you feel like some sort of Ubermensch, nor are they supposed to make you Always Feeling Good, they are meant to restore normal emotional functioning.
I somehow doubt you were prescribed 875mg of amphetamine salts a day. If the pharmacist saw a script for that I'd bet they'd laugh you out of the pharmacy. The highest dose of Adderall that is manufactured is a measly 30mg so you'd need to have your monster caps custom-made. If you were taking almost a gram of amphetamine per day, then you'd absolutely need a solid whack of phenobarbital to put you to sleep. I'd also be amazed if you didn't go off the rails and go totally bonkers either. People who take "heroic" doses of amphetamines have this unfortunate tendency to eventually neglect diet and sleep to the point where your mind just implodes into itself and the Shadow People are trying to convince you to kill your family.
Nowadays amphetamine is only rarely if ever prescribed as an antidepressant. It would be more accurate to say that at such high dosages it's more of a recreational euphoriant drug than a true antidepressant. Antidepressants are not supposed to make you feel like some sort of Ubermensch, nor are they supposed to make you Always Feeling Good, they are meant to restore normal emotional functioning.
- Joined
- Jul 2, 2008
- Messages
- 9,131
Various dementias. But tbh MAO-B inhibitors are usually used on the side.
Yeah ketamine is somewhat of an enigma, but yes.
I have heard that there used to be pills with a stupid amount of amphetamine in them, in the past. I can't verify that. I don't know the history. Thoughts? Dare I ask for source(s)??
Since the max dose allowed is now just the recommended max dose allowed, people do take more than 60. There was one source saying that 1/3 of users need more than 60, and that scripts reach 500mg. For the former, I doubt it, as everyone with ADHD whom I've met isn't taking 30mg without patient "intervention". And the latter, toxic at least.
People forget that the chemical both accumulates in one's brain and reaches new brain regions in density as this process continues, and that it's really very rarely actually supposed to make you happy. A proper dose usually would not bear on mood.
It's kind of an age-old tactic to offer stimulants as augmentation for depression treatment, but as last-resort these days. Lithium, and even ECT come before. ECT, no thanks sorry doc I need my brain.
I can say that, if you take breaks, it can work on mood to a limited extent, but that's taking it 1-3 times per week. But people have to stop thinking it will make them miraculously happy at one constant dose.
Apparently in older people it's more viable for mood. I could see this, if just for how it stimulates hormonal activity.
But meditation and working out have a better place in my heart than speed.
Yeah ketamine is somewhat of an enigma, but yes.
I have heard that there used to be pills with a stupid amount of amphetamine in them, in the past. I can't verify that. I don't know the history. Thoughts? Dare I ask for source(s)??
Since the max dose allowed is now just the recommended max dose allowed, people do take more than 60. There was one source saying that 1/3 of users need more than 60, and that scripts reach 500mg. For the former, I doubt it, as everyone with ADHD whom I've met isn't taking 30mg without patient "intervention". And the latter, toxic at least.
People forget that the chemical both accumulates in one's brain and reaches new brain regions in density as this process continues, and that it's really very rarely actually supposed to make you happy. A proper dose usually would not bear on mood.
It's kind of an age-old tactic to offer stimulants as augmentation for depression treatment, but as last-resort these days. Lithium, and even ECT come before. ECT, no thanks sorry doc I need my brain.
I can say that, if you take breaks, it can work on mood to a limited extent, but that's taking it 1-3 times per week. But people have to stop thinking it will make them miraculously happy at one constant dose.
Apparently in older people it's more viable for mood. I could see this, if just for how it stimulates hormonal activity.
But meditation and working out have a better place in my heart than speed.
SlowandFastandSlow
Bluelighter
- Joined
- Jan 21, 2020
- Messages
- 77
Amphet for depression seems like it was just "it makes you feel better? It works!" All good untill tolerance or you run out.
Plus phet makes you unstable to fuck in the long run.
Honestly if I had unlimited funds and a perfect connect cocaine would probably be a pretty damn effective anti-depressant so long as you kept the doses limited.
I always wonder what the effects on depression would be from some kinda slow release cocaine along the lines of concerta, I realise it wouldn't actually be viable as a treatment but still interesting.....
Plus phet makes you unstable to fuck in the long run.
Honestly if I had unlimited funds and a perfect connect cocaine would probably be a pretty damn effective anti-depressant so long as you kept the doses limited.
I always wonder what the effects on depression would be from some kinda slow release cocaine along the lines of concerta, I realise it wouldn't actually be viable as a treatment but still interesting.....
Iceman1216
Bluelighter
- Joined
- Feb 27, 2019
- Messages
- 1,056
I like Lexapro!! Has saved my mental health, for the last few years. Only thing I really dislike about SSRI is how hard it diminishes Sex Drive!!
SlowandFastandSlow
Bluelighter
- Joined
- Jan 21, 2020
- Messages
- 77
I think anything that increases seretonin long term does that though, no?
- Joined
- Jul 2, 2008
- Messages
- 9,131
Most instances of depression respond to serotonergic agents, but not all. There's also the question of does increasing serotonin lead to remittance, or reduction of it (after initial spike) and resultant transcription factors, the latter which seems more likely given that it takes some time to work.
Cocaine is too cardio-toxic to use regularly forever, and to a lesser extent neurotoxic.
Cocaine is too cardio-toxic to use regularly forever, and to a lesser extent neurotoxic.
polymath
Bluelight Crew
- Joined
- Nov 4, 2010
- Messages
- 1,884
There are many different mechanisms that an antidepressant could have, including
- kappa receptor blocker
- substance P antagonist
- something endocannabinoid related, like the antidepressant effect of acetaminophen
- delta agonists (the effects of SSRIs are partly blocked with delta antagonists, so they may have a downstream effect on delta receptors)
All of these seem to have surprisingly little side effects, but none of them are in clinical use yet.
Edit: The orphenadrine molecule has a diphenylmethyl group connected to an oxygen, then two carbon atoms between the oxygen and the nitrogen atom. This is similar to benztropine, except that in it there are three carbons between O and N.
In the case of benztropine, putting 4-chloro or 3,4-dichloro substituents on one of the aromatic rings increases the DAT affinity significantly, but doesn't necessarily make the molecule have any "recreational" value.
- kappa receptor blocker
- substance P antagonist
- something endocannabinoid related, like the antidepressant effect of acetaminophen
- delta agonists (the effects of SSRIs are partly blocked with delta antagonists, so they may have a downstream effect on delta receptors)
All of these seem to have surprisingly little side effects, but none of them are in clinical use yet.
Edit: The orphenadrine molecule has a diphenylmethyl group connected to an oxygen, then two carbon atoms between the oxygen and the nitrogen atom. This is similar to benztropine, except that in it there are three carbons between O and N.
In the case of benztropine, putting 4-chloro or 3,4-dichloro substituents on one of the aromatic rings increases the DAT affinity significantly, but doesn't necessarily make the molecule have any "recreational" value.
Last edited:
Bravoncius Roxford
Bluelighter
- Joined
- Feb 1, 2017
- Messages
- 105
If you were 'deficient in dopamine' you would present with Parkinsons, not depression.
This argument is a little silly. The amount of dopamine needed for normal movement is minimal: you need to lose something like 70% of all your dopaminergic neurons in the substantia nigra for you to develop the symptoms of Parkinson's. There is enormous benefit for one's mood from having higher-than-"normal" dopamine levels. I can present as evidence people that carry the single-nucleotide polymorphism of the COMT gene Val158Met, which results in the substitution of a valine for a methionine. This makes the enzyme far less stable at the human body temperature of 37 centigrade, and the enzyme cannot do it's job as effectively. This results in significantly impaired catabolism of catecholamines and levodopa. The higher availability of dopamine results in enhanced mood: people with this nucleotide mutation report over twice the amount of positive emotions compared to people who carry the normal variant of the enzyme. https://pubmed.ncbi.nlm.nih.gov/17687265
Also, you are wrong about dopamine and depression. I suggest you check the works of Ken Gillman, who is both a pharmacologist and psychiatrist with over 30 years of experience. He postulates that depression, especially severe endogenous depression, is mostly caused by malfunctioning of the dopaminergic and opioidergic systems of the brain,. which is why the SSRIs and SNRIs are not very effective for truly depressed people and why the rates of remission are so low. Also, the role of dopamine is not recognized and dopaminergics are being used to treat serious depression.
Nowadays amphetamine is only rarely if ever prescribed as an antidepressant. It would be more accurate to say that at such high dosages it's more of a recreational euphoriant drug than a true antidepressant. Antidepressants are not supposed to make you feel like some sort of Ubermensch, nor are they supposed to make you Always Feeling Good, they are meant to restore normal emotional functioning.
This is also not technically accurate. Serotonergic antidepressants only rarely raise mood above "normal", true. But the reason why antidepressants almost never make one even slightly euphoric is because most antidepressants work via serotonin, and serotonin is a chemical mostly related to perceptions of resource availability, and thus mediate mostly anxiety and apprehension. High levels of serotonin tend to dull emotions. It reverses depression by decreasing the "tone" of emotional response.
But that antidepressants rarely make you feel euphoric is due to the fact that most antidepressants are serotonergic and not because there is something magical about antidepressants that restore "normal" mood but don't make you feel good. Back in the 1970's there were two antidepressants, nomifensine and amineptine, which were notorious for inducing mild euphoria. They made people feel slightly euphoric because they are inhibitors of the reuptake of norepinephrine and dopamine. That is, their mechanism of action was similar to cocaine, although with weaker adrenergic action. The non-selective MAOIs are also notorious for making people feel "better than well", and the reason for that, among other things, is that they increase norepinephrine and dopamine and not only serotonin. In fact, that the MAOIs increase dopamine is the reason why Dr.Gillman favors tranylcypromine and phenelzine over all other antidepressants for treating serious depression.
polymath
Bluelight Crew
- Joined
- Nov 4, 2010
- Messages
- 1,884
But that antidepressants rarely make you feel euphoric is due to the fact that most antidepressants are serotonergic and not because there is something magical about antidepressants that restore "normal" mood but don't make you feel good. Back in the 1970's there were two antidepressants, nomifensine and amineptine, which were notorious for inducing mild euphoria. They made people feel slightly euphoric because they are inhibitors of the reuptake of norepinephrine and dopamine. That is, their mechanism of action was similar to cocaine, although with weaker adrenergic action. The non-selective MAOIs are also notorious for making people feel "better than well", and the reason for that, among other things, is that they increase norepinephrine and dopamine and not only serotonin. In fact, that the MAOIs increase dopamine is the reason why Dr.Gillman favors tranylcypromine and phenelzine over all other antidepressants for treating serious depression.
The problem with this is that it can make people hyperactive and sexually promiscuous in a way that family members find disturbing... One of the things that are a problem just because not everyone is like that.
Some people have synthesized combined mu agonist/substance P antagonist compounds, and then there doesn't seem to develop tolerance to the opioid effect. Make that a kappa receptor blocker too, and you'd have a great antidepressant.
Bravoncius Roxford
Bluelighter
- Joined
- Feb 1, 2017
- Messages
- 105
The problem with this is that it can make people hyperactive and sexually promiscuous in a way that family members find disturbing... One of the things that are a problem just because not everyone is like that.
First, that is for the person to decide and not the family. Secondly, I will take being active and having a strong sex drive over being apathetic to the point I won't even move and important any day of the week.
Some people have synthesized combined mu agonist/substance P antagonist compounds, and then there doesn't seem to develop tolerance to the opioid effect. Make that a kappa receptor blocker too, and you'd have a great antidepressant.
We already have that, tianeptine, which has recently been proven to be a pretty strong agonist of the human Mu opioid receptor. And guess what? Tianeptine has been extensively abused to the point where European authorities are seriously considering removing it from the market. And yes, it does produce physical dependence and has the worst withdrawal of any antidepressant. So you are wrong on all counts.
polymath
Bluelight Crew
- Joined
- Nov 4, 2010
- Messages
- 1,884
^ The so called "normal" people tend to see problems in many things where no one who writes on this forum sees them.
I can't see anything being said anywhere about tianeptine being a substance P (neurokinin 1 receptor) antagonist. If blocking that receptor really prevents opioid tolerance, a combined mu partial agonist and NK1R blocker could have a long term antidepressant effect. Make it a weak enough partial agonist and it would be impossible to get too intoxicated with it.
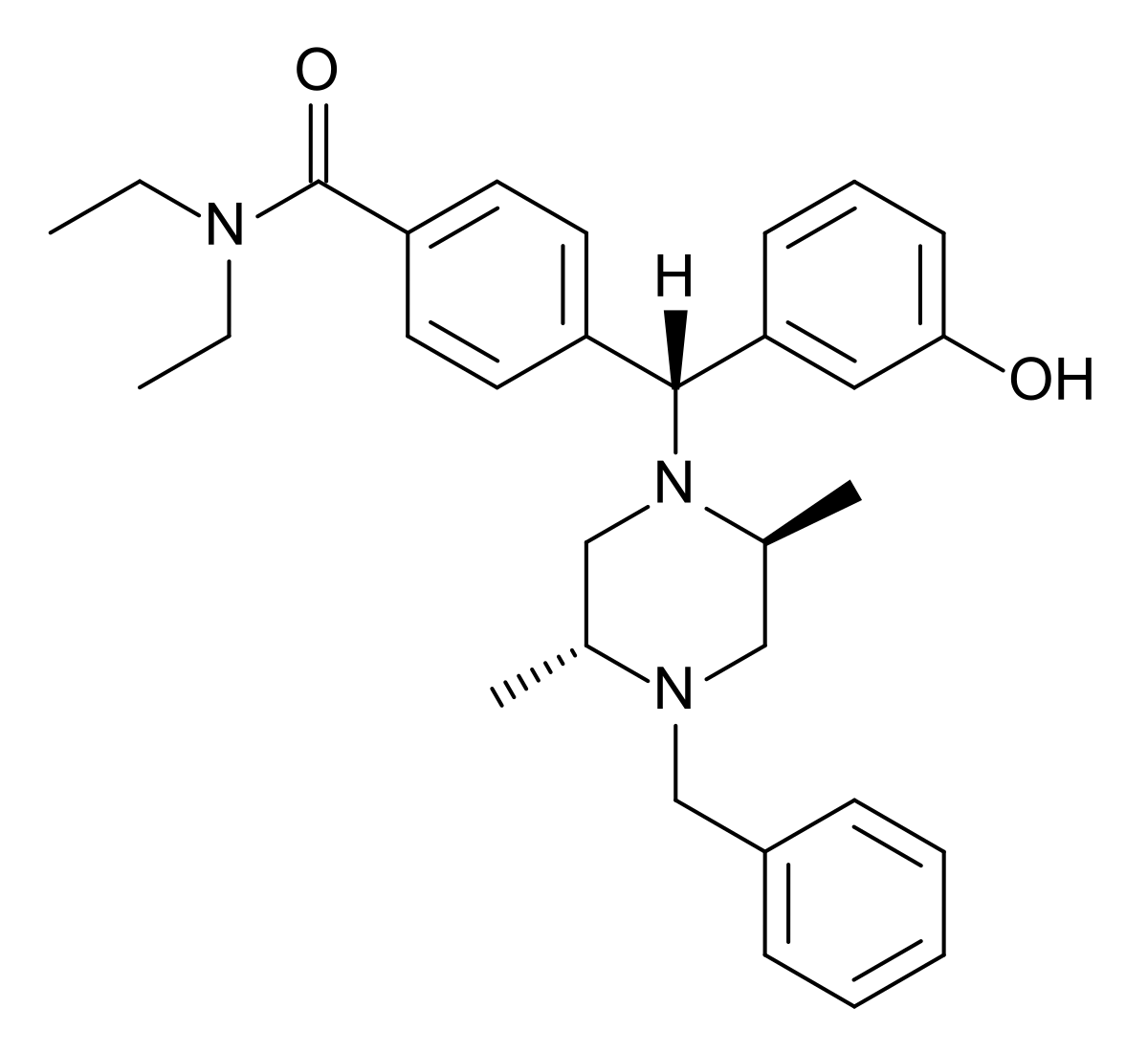
Edit: Many of the selective delta-opioid agonists seem to have this same diphenylmethyl group as in many antihistamines.
 en.wikipedia.org
en.wikipedia.org

If tripelennamine and others were to bind to the delta receptor, it could explain why the mixture of pentazocine and tripelennamine was considered euphoric by some people. A combined kappa-delta agonist can produce analgesia without dysphoria and anxiety: http://europepmc.org/article/PMC/4651729
I can't see anything being said anywhere about tianeptine being a substance P (neurokinin 1 receptor) antagonist. If blocking that receptor really prevents opioid tolerance, a combined mu partial agonist and NK1R blocker could have a long term antidepressant effect. Make it a weak enough partial agonist and it would be impossible to get too intoxicated with it.
Edit: Many of the selective delta-opioid agonists seem to have this same diphenylmethyl group as in many antihistamines.
DPI-287 - Wikipedia
If tripelennamine and others were to bind to the delta receptor, it could explain why the mixture of pentazocine and tripelennamine was considered euphoric by some people. A combined kappa-delta agonist can produce analgesia without dysphoria and anxiety: http://europepmc.org/article/PMC/4651729
3-Iodobenzoyl naltrexamine (IBNtxA) is a potent analgesic belonging to the pharmacologically diverse 6β-amidoepoxymorphinan group of opioids. We present the synthesis and pharmacological evaluation of five analogs of IBNtxA. The scaffold of IBNtxA was modified by removing the 14-hydroxy group, incorporating a 7,8 double bond and various N-17 alkyl substituents. The structural modifications resulted in analogs with picomolar affinities for opioid receptors. The lead compound (MP1104) was found to exhibit approximately 15-fold greater antinociceptive potency (ED50 = 0.33 mg/kg) compared with morphine, mediated through the activation of kappa- and delta-opioid receptors. Despite its kappa agonism, this lead derivative did not cause place aversion or preference in mice in a place-conditioning assay, even at doses 3 times the analgesic ED50. However, pretreatment with the lead compound prevented the reward behavior associated with cocaine in a conditioned place preference assay. Together, these results suggest the promise of dual acting kappa- and delta-opioid receptor agonists as analgesics and treatments for cocaine addiction.
Last edited: