paracelsius
Bluelighter
- Joined
- Mar 11, 2020
- Messages
- 197

So I took a close look at the OP compound aka anazocine discussed some time ago. Quite possibly one of the most euphoric OP (AND stim!) known to man. Or at least one of the most addictive. Afaik, it is one of the very very few compounds that morph-trained macaque monkeys would gladly prefer it to IV morph (from that japanese study mentioned in previous thread). I mean by day 30, the monkeys were self-IVing it at a whopping rate of 300 times a day (20mg/kg dose)..300x/day!! basically non-stop dosing themselves 24/7! Which means huge tolerance develop quickly, but surprising they didn't OD (up to 150mg/kg IV in OP-naive animals, they did fine according to the authors.. expect I could only imagine the euphoria at that huge dose
") .. more like IV-ing cocaine AND heroin at the SAME time..why I say that? read-on
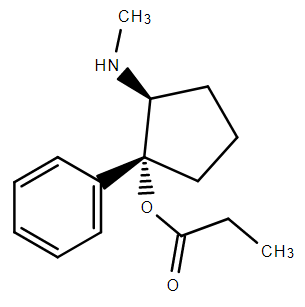
.. more like IV-ing cocaine AND heroin at the SAME time..why I say that? read-onI been trying to see why is this compound so addictive? well it turns out, as I read that old japanese paper, the original synth actually gives a 30:70 ratio of the cis and trans isomer (from the reaction of the corresponding bicyclic ketone with phenyl-grignard).
Now, if you look closely, the trans isomer superimposes neatly (>80% ) to the cocaine analog Troparil, a DNRI, and the cis isomer superimposes to the mu-opioid agonist ketobemidone or to demerol. So in other words, the trans isomer is (very likely imo) a DNRI (as potent as cocaine?) and the cis a mu-Opioid agonist (~4x more potent than morph found by those studies). Quick swisstarget prediction predicts Serotonin Norepinephrine Dopamine Transporters, Sigma and mu-Opioid as the top 5 most likely targets (which is what I suspect). In other words it is a mu-opioid agonist and (most likely) a SDNRI as well.
So basically I think what those guys were dealing with was the ultimate speed-ball (the 30:70 mixture of cis-trans isomers) with the trans isomer acting as a stim as potent as cocaine (more I would say, probably 5-10x more, from troparil-type cocaine analogs SAR) and the cis isomer acting as a mu-OP agonist (~4x morph) within similar dosing range.
I mean, the ED50s for SDNRI and mu-opioid agonism are probably within same range so the dose will activate both SNDRI and mu-OP at the same time!! that's an opinion tho (data for SDNRI not done afaik only that of mu-OP, analgesia and locomotor in rats and macaques). This probably explains why the monkeys didn't OD, SNDRI activity counteracting OP respiratory depression, making it "safer" than pure OPs like fent, but way much more euphoric and addictive!? .. Now, I don't know about the SNDRI of that chem (that hasnt been done afaik, just comparing the trans compound with troparil on paper)..
But I would bet my last shirt, trans-Anazocine is a potent, cocaine-like Serotonin-Dopamine-Norepinephrine Reuptake Inhibitor and cis-Anazocine a potent mu_opioid agonist and the reason monkeys prefer it to IV-morph is probably due to that: they were basically speed-balling non-stop on 20mg/kg of the drug .. have a good'day y'all BLighters....
Last edited: