3. Brain/Neuron
This chapter is to prepare you for the next one about different important receptors.
Now most of the effects of psychoactive drugs take place in this squishy pinkish/grey organ called brain. The brain takes about 2% of the body-weight and consumes quite a lot of glucose for its weight. The brain is divided into two hemispheres, the left and right one, connected via commissural nerve tracts, with the corpus callosum being the largest.
The brain consists of various different cells, the primary ones being neurons, glia cells and blood vessels.
For us the neuron is the most important one as that's where the fun takes place. The neuron is a cell that can be electrically excited and receives, processes and transmits information using electrical and chemical signals. Its structure consists of a cell body, also called soma, with dentrites and an axon (usually wrapped in myelin sheat) with axon terminals. Usually a signal is received via the dendrites leading to the soma, the fate of the signal (either transmission or no transmission) is chosen at the axon hillock. From there the signal travels to the axon terminals. This is where the synapse is located.
3.1 Synapse
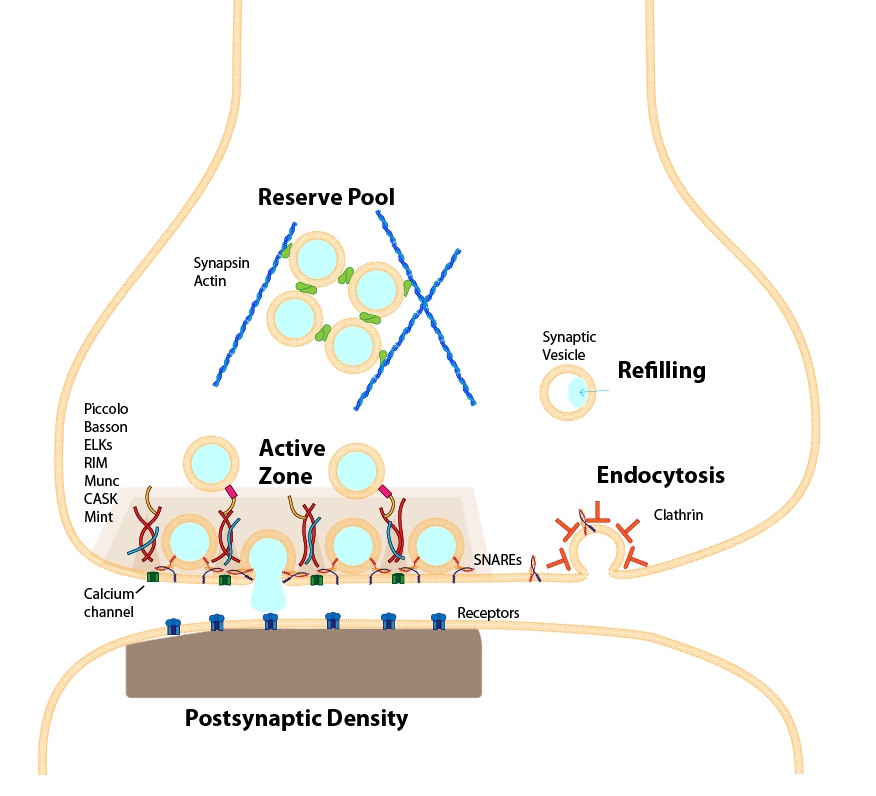
https://upload.wikimedia.org/wikipedia/commons/1/10/Active_zone3.JPG
The synapse is a structure found between neurons that permits those neurons to communicate via chemical signals. It consists of the pre-synapse (= axon terminal), the synaptic cleft and the post-synapse (= dendrite). Now besides this classical axodentritic synapse there are other arrangements like axosecretory (the axon terminal secretes substances directly into the bloodstream) and axoaxonic (the axon terminal secretes into another axon) for example.
3.2 Potential
Now that we understand the structure let's try to understand the processes involved in signaling. As you might remember we learned that the neuron can be electrically excited. I'll now explain how this works.
A cell, like the neuron, is sealed from the outside by the cell membrane. Now there's a difference in voltage due to different ions, the most important ones being sodium, potassium, chloride and calcium, and other stuff, like proteins (usually slightly negatively charged) between the inside of the cell and the outside. This is the reason for the (resting) membrane potential. A typical voltage across a membrane is around -75 mV (resting potential), meaning that the inside of the cell has a negative voltage relative to the outside as long as nothing perturbs the cell.
But as we learned the membrane is packed with different transporters and channels that are able to transport ions and other molecules.
This leads us to the action potential:
The action potential is a temporary shift in the membrane potential from negative to positive due to influx and efflux of different ions.
In the resting phase the two types of voltage gated ion channels, potassium and sodium, are closed. If a stimulus now leads to an increase in voltage and once a certain threshold is reached the voltage gated sodium channels are opened. This leads to a flow of positively charged sodium ions inside the neuron, thus resulting in a positive inside. This phase is called depolarization. Once a voltage of around +40 mV is reached the voltage gated sodium channels will be shut down and inactivated. At the same time voltage gated potassium channels are opened. Positively charged potassium rushes out of the neuron making the inside more negative again. This phase is called repolarization. As the voltage gated potassium channels need some time to close again the potential overshoots to around -90 mV (after hyperpolarization). To get back to the resting potential (-75 mV) the neuron uses Na+/K+ ATPase pumps moving 3 Na+ out and 2K+ ions inside the cell.
Remember the structure of the neuron? Many signals from other neurons arrive at the dendrites, those signals can either.
3.2.1 EPSP and IPSP
So now that we understand the structure of a synapse and how the resting and action potential work we can put it together to understand EPSP (excitatory postsynaptic potential) and IPSP (inhibitory post synaptic potential).
If you remember the structure of a synapse it starts with dendrites. Here's where the EPSPs and IPSPs happen.
An action potential in the pre-synapse leads to the release of neurotransmitters into the synaptic cleft. Those neurotransmitters bind to receptors on the post-synaptic membrane and lead to either an EPSP or IPSP.
Action potentials are all or nothing signals that usually start at the axon hillock. Both excitatory and inhibitory signals from the dendrites are added up and if the excitatory signals exceed the inhibitory an action potential arises at the axon hillock making it's was to the axon terminal where it triggers the release of vesicles with neurotransmitters into the synaptic cleft to trigger an EPSP or IPSP in the downstream neuron.
Glutamate is the most common neurotransmitter associated with EPSP and GABA with IPSP.
3.3 Ligands
3.3.1 Agonist
An (full) agonist is a substance that has an affinity to a certain receptor, binds to this receptor and activates (intrinsic activity) the receptor producing a biological response.
3.3.2 Antagonist
An antagonist is a substance that has an affinity to a certain receptor, binds to this receptor but produces no effects (no intrinsic activity). Another word for antagonist would be blocker, as it block the receptor without activating it. The activity can be reversible (binds to a receptor or enzyme only for a certain period of time) or irreversible (certain MAOIs bind irreversible to the monoaminooxidase rendering the enzyme worthless, so your body has to produce new, functioning enzymes). Antagonists can be competitive (bind to the same binding site as the endogenous ligand/agonist thus competing for the binding site) or non-competitive (doesn't compete for binding either by binding to the receptor irreversibly/nearly irreversible or by binding to another site, this would be called an allosteric antagonist).
3.3.3 Partial agonist
A partial agonist is a substance that has an affinity to a certain receptor, binds to this receptor and activates (intrinsic activity) the receptor, but only partially, producing a biological response lesser than a full agonist. To visualize it think of it this way: We have 100 receptors, a full agonist has a 100% chance of activating the receptor, so by taking a full agonist we activate all 100 receptors. Now a partial agonist has only for example a 50% chance of activating the receptor, so by taking a full agonist we activate on average only 50 receptors.
This can be a problem with certain drugs, like buprenorphine. If you're physically dependent on a full agonist, like morphine, but want to switch to bupe there's something called precipitated withdrawal due to the fact that bupe is only a partial agonist with a high affinity for the mu-opioid receptor. If you take the bupe too soon after taking morphine the bupe will bind to the opioid receptors due to the high affinity but only activate them to a partial extend, leaving you in withdrawal as you're used to the full activation. This can be bypassed by waiting a certain time (check out the COWS score) before buprenorphine induction.
3.3.4 Inverse agonist
An inverse agonist is a substance that has an affinity to a certain receptor, binds to this receptor but induces a response opposite to that of an agonist. This one takes some time to understand, so bear with me. A precondition for a inverse agonist is that the receptor it binds to has something called basal activity, this simply means that there's a certain chance that the receptor spontaneously, without the binding of an agonist, activates itself. Now with that in mind it's easier to understand. The inverse agonist binds to the receptor but instead of activating it, it decreases the activity below the basal level, by decreasing the chance of the receptor activating itself.
If you haven't fully understand this yet let me explain it by using an example. Let's take receptor X with a basal activity of 10 activations a minute. By adding an inverse agonist we decrease the activity from 10 activations a minute to say 2 activations a minute. So the inverse agonist has a negative intrinsic activity.