
basement_shaman
Bluelighter
- Joined
- Dec 14, 2010
- Messages
- 168
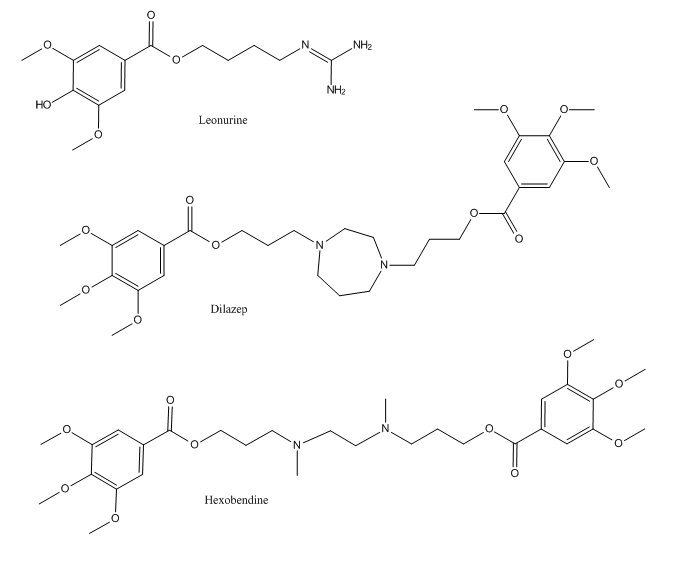
I have been comparing the molecular structure of leonurine, the principal alkaloid from Wild dagga, Klip dagga etc. in order to find structural similarities with an existing drug with a known pharmacological profile.
I finally hit a gold mine: two of the existing adenosine reuptake inhibitors are basically two molecules of leonurine stitched together at the double amine tail (save for a hydroxyl group being substituted for by a methoxy group.)
Take a look!
Do you think my hypothesis that leonurine acts as an adenosine uptake inhibitor is complete bullshit, or could there be some truth to it?
Caffeine, an adenosine receptor competitive antagonist, should then antagonize the effects leonurine, which makes the hypothesis easily testable by bioassays. I just smoked myself retarded in wild dagga, and I'm now going to down a few glasses of cola. But my results will mean nothing scientifically, they will only be mildly interesting at best. Hopefully a real study will be carried out one day.
Edit: as additional circumstantial evidence for my hypothesis, leonurine has been shown to protect against all kinds of ischemias1 2, which adenosine also does3 4.
Source 1
Source 2
Source 3
Source 4
I finally hit a gold mine: two of the existing adenosine reuptake inhibitors are basically two molecules of leonurine stitched together at the double amine tail (save for a hydroxyl group being substituted for by a methoxy group.)
Take a look!
Do you think my hypothesis that leonurine acts as an adenosine uptake inhibitor is complete bullshit, or could there be some truth to it?
Caffeine, an adenosine receptor competitive antagonist, should then antagonize the effects leonurine, which makes the hypothesis easily testable by bioassays. I just smoked myself retarded in wild dagga, and I'm now going to down a few glasses of cola. But my results will mean nothing scientifically, they will only be mildly interesting at best. Hopefully a real study will be carried out one day.
Edit: as additional circumstantial evidence for my hypothesis, leonurine has been shown to protect against all kinds of ischemias1 2, which adenosine also does3 4.
Source 1
Source 2
Source 3
Source 4
Last edited:


") [/non-ADD material haha]
[/non-ADD material haha]