Apparently BigPharma has come up with non-cardiotoxic analogs of ibogaine -type psychedelic alkaloids for opiates withdrawal/treatment (they'll probably be charging a $100,000 a pill..) does anyone come across any structures related to those?.. thx4posting..
-
N&PD Moderators: Skorpio | thegreenhand
-
Neuroscience & Pharmacology Discussion Welcome Guest
Posting Rules Bluelight Rules Recent Journal Articles Chemistry Mega-Thread FREE Chemistry Databases! Self-Education Guide
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Non-cardiotoxic Ibogaine psychedelic analogs
- Thread starter DotChem
- Start date
S.J.B.
Bluelight Crew
- Joined
- Jan 22, 2011
- Messages
- 6,886
There aren't any FDA-approved drugs for opioid withdrawal based on ibogaine's structure. The only analogue I could find with a decent amount of recent clinical study is noribogaine - an active metabolite of ibogaine - but it seems to have similar cardiovascular effects to the parent molecule. There's also a recent patent on noribogaine analogues as potential withdrawal medicines by Florida's DemeRx, a small biotech company.
Where did you hear about these non-cardiotoxic analogues? I would be curious to find out more as well.
Where did you hear about these non-cardiotoxic analogues? I would be curious to find out more as well.
^ You're absolutely right. There are no FDA approved drugs based on Iboga structure.. Only Noribogaine (main metabolite of Ibogaine) and also 18-MC that have some clinical data. Main reason of lack of clinical data being Ibogaine is classified Schedule I so you won't find any studies from the US and even less any compounds under consideration for approval by FDA..
Anyway, like you mentioned, Noribogaine (and also 18-MC) are also cardiotoxic, like Ibogaine ie they induce hERG prolongation, cardiac arrhythmia that could lead to sudden death in some individuals with preexisting heart problems at therapeutically relevant concentrations (Mechanism of hERG Channel Block by the Psychoactive Indole Alkaloid Ibogaine). So they have no real advantages over plain Iboga Roots Barks extracts. What I was talking about, at a conference in Singapore last spring, a Canadian biotech company claimed to have developed Iboga-type isoquinuclidine compounds that DO NOT HAVE hERG liabilities at therapeutically relevant doses but have same anti opiates withdrawal/craving properties as Ibogaine.
But they did not disclose any structures tho only code name of their compounds they are studying.. So I thought someone might have come across some of those.. Only recent patent I can find on Ibogaine analogs is this one (from Columbia University).. It claimed lots of compounds I mean really broad range of Iboga type isoquinuclidines.. could possibly be some of these compounds, who knows?? .. I'll post update later when I learn anything about this.. thx
Anyway, like you mentioned, Noribogaine (and also 18-MC) are also cardiotoxic, like Ibogaine ie they induce hERG prolongation, cardiac arrhythmia that could lead to sudden death in some individuals with preexisting heart problems at therapeutically relevant concentrations (Mechanism of hERG Channel Block by the Psychoactive Indole Alkaloid Ibogaine). So they have no real advantages over plain Iboga Roots Barks extracts. What I was talking about, at a conference in Singapore last spring, a Canadian biotech company claimed to have developed Iboga-type isoquinuclidine compounds that DO NOT HAVE hERG liabilities at therapeutically relevant doses but have same anti opiates withdrawal/craving properties as Ibogaine.
But they did not disclose any structures tho only code name of their compounds they are studying.. So I thought someone might have come across some of those.. Only recent patent I can find on Ibogaine analogs is this one (from Columbia University).. It claimed lots of compounds I mean really broad range of Iboga type isoquinuclidines.. could possibly be some of these compounds, who knows?? .. I'll post update later when I learn anything about this.. thx
Last edited:
mr peabody
Bluelight Crew
- Joined
- Aug 31, 2016
- Messages
- 5,714
According to one report from the NY Academy of Sciences, "Ibogaine, but not 18‐MC, decreases heart rate at high doses." Is this wrong?
https://nyaspubs.onlinelibrary.wiley.com/doi/full/10.1111/j.1749-6632.2000.tb05211.x
Also,
"Hurst says that so far, it appears that 18-MC is what it promised to be. The first round of testing in rats showed no cardiovascular or psychedelic effects..."
https://www.csindy.com/coloradospri...to-heroin-and-other-drugs/Content?oid=3927464
If you already know the answer, I won't keep looking.")
https://nyaspubs.onlinelibrary.wiley.com/doi/full/10.1111/j.1749-6632.2000.tb05211.x
Also,
"Hurst says that so far, it appears that 18-MC is what it promised to be. The first round of testing in rats showed no cardiovascular or psychedelic effects..."
https://www.csindy.com/coloradospri...to-heroin-and-other-drugs/Content?oid=3927464
If you already know the answer, I won't keep looking.
Last edited:
You right.. 18-MC may (MAY) be less cardiotoxic than Ibogaine or noribogaine..
edit: that company was claiming Iboga analogs pretty much devoid of hERG affinity ie IC50>200mg/kg in rats which roughly translate to ~40mg/kg in humans (3-5 gram doses) which are way higher than flood doses (1-2g).. should anybody come across structures of such compounds.. thx4posting
Then again, we know about Ibogaine "flood" doses and cardiac arrythmia in humans but nothing about 18-MC "flood" doses.. could well be safer than Ibogaine in humans.. who knows??The Anti-Addiction Drug Ibogaine and the Heart: A Delicate Relation......Is the Ibogaine Congener 18-MC Less Cardiotoxic than Ibogaine?
In contrast to ibogaine, even high doses of 18-MC did not show any apparent effects on either heart rate or blood pressure in animal experiments [4]. We have previously shown that the affinity of 18-MC to human cardiac voltage-gated ion channels is lower than that of ibogaine [17]. In principle, these findings imply a reduced risk for cardiac adverse effects for 18-MC in comparison with ibogaine application. However, 18-MC’s affinity for hERG channels (IC50, 15 μM) is still near to the therapeutic concentration range (see above), if similar plasma protein binding as for ibogaine is assumed. Thus, like ibogaine, 18-MC may have the propensity to induce QT interval prolongation and TdP arrhythmias. A recent study from Alper’s group [63] also suggested that 18-MC shows lower affinity for hERG channels than ibogaine. Here, the IC50 for hERG current inhibition was estimated to lie between 50 and 100 μM, a value considerably higher than we reported in [17]. Together, these studies suggest that, compared with ibogaine, 18-MC is less cardiotoxic, and has a lower propensity to induce TdP arrhythmias when applied in similar concentrations. The lack of knowledge about the amount of 18-MC’s plasma protein binding, however, is an element of uncertainty which remains.
edit: that company was claiming Iboga analogs pretty much devoid of hERG affinity ie IC50>200mg/kg in rats which roughly translate to ~40mg/kg in humans (3-5 gram doses) which are way higher than flood doses (1-2g).. should anybody come across structures of such compounds.. thx4posting
mr peabody
Bluelight Crew
- Joined
- Aug 31, 2016
- Messages
- 5,714
Wow, what a great paper. I've now condensed the salient points here: http://www.bluelight.org/vb/threads...iate-opioid-addiction?p=14383433#post14383433
BTW, I've been collecting reports about daily low dosing iboga (wonder if you might have an interest in that). Anyway, here are some (sorry to throw all this stuff at you willy-nilly):
Ibogaine has also been given in regimens of small daily doses of 25 to 300 mgs/day and in small daily doses where the dose is increased on a daily basis until the desired interruption of drug dependence is accomplished. These low dose modalities have not been validated for efficacy, however, they can be traced back some decades to the work of Leo Zeff who in the case of a single patient provided ibogaine on an "as needed" basis via nasal administration to a cocaine dependent patient to substitute for his cocaine use. Lines of ibogaine were somewhat equivalent to lines of cocaine, and the patient ceased cocaine use after a week of this daily self-regulated ibogaine regimen. Additionally, reports from Canadian sources indicate multi-week low dose ibogaine therapy 20 mg/day following a therapeutic dose of ibogaine in the treatment of cocaine dependence. Further, reports throughout the ibogaine provider community indicate the use of multiple dosing of varying strength doses over varying time periods in the treatment of opioid dependence. As with all determinations in medicine, decisions must be made based on observations of the patient and knowledge of the disorder(s) and the medication(s) used.
From the "Manual for Ibogaine Therapy Screening, Safety, Monitoring & Aftercare" by Howard S. Lotsof & Boaz Wachtel: http://ibogainedossier.com/manual.html
-----
There are 3 main options for ibogaine treatment (*these are all after a small test dose)
– single administration of 1 high dose ibogaine (with booster doses over the next few days/weeks if needed)
– single day/night of administration of multiple large doses spaced out by a few hours (with booster doses over the next few days/weeks as needed)
– small daily doses of 25-300 mg/day, where the dose is gradually increased each day until it is felt to have been effective for eliminating WDs/cravings (this one can be modified quite a bit)
http://www.dialogue.space/ibogaine-help-and-advice/
-----
Yes, small dosages are beneficial too, if one for example would like to deal just with the cravings. Not really sure though if Dr Mash`s theory of the effect of ibogaine metabolite (nor-ibogaine) staying long in the body really explains ibogaine`s long-term effects. It`s possible for example to take 200mg of Ibo HCl a week, or up to 50 mg a day...it`s very individual. Just don`t try the row powder from the iboga root - very harsh and very little effect.
http://archive.li/PMNzW
-----
My big bright idea, is to dose on opiates/opioids, and then take iboga root...but take a VERY small dose of iboga alkaloids, on a daily basis. and see if over time the iboga creates a potentiation of the opiate dose, allowing for reduction of the daily amount of opiates being used. I know one hypothesis is that the long lasting iboga metabolites cause part of the reduction/abolishment of opiate withdrawl...my idea hinges on this active metabolite hypothesis. The thought that a large, potentially dangerous, and mentally exhaustive standard iboga/ibogaine dose might be stretched out over a multitude of days and still create an active metabolite that has therapeutic value might appeal to people that are not ready for entry into a mindbending, physically taxing arena.
http://archive.li/PMNzW
-----
[Ibogaine] Ataxia and involuntary muscle movements induced by small daily doses interacting with other meds
I am posting this to the list in case anyone else may have had experience in this area and that hasn't posted it, and as an alert to others in case they see something like what I am about to describe develop. A client has been taking very small doses of ibogaine hcl (10-mg) once daily for approximately one month, to build up their nor-ibogaine levels so as to reduce tolerance to prescription pain medications. At the time the following symptoms emerged, the medication list included dilaudid (16mg q.i.d.), morphine sulfate (10mg as needed for breakthrough pain, about 3-4x daily), amphetamine (30-mg as needed to combat drowsiness of narcotics), Naprelan (Naprosyn extended release for mild arthritis), and Clonazepam (2-mg b.i.d.). A one-day trial of Trileptol (one dose) was initiated to possibly reduce the neuropathic pain being treated by the narcotics, but since this just made the client excessively sleepy it was not continued.
The client had not taken any amphetamine for approximately 2 weeks after initiating the ibogaine. About 4 days after initiating a small amount of amphetamine, the client developed involuntary muscle movements affecting the limbs and face. This included facial grimacing and eye rolling, as well as ataxia and loss of balance, including involuntary leg movements (bending at the knee and raising of the legs behind), arm movements, and sudden leg movements both forward and backwards. Since these movements were involuntary and obviously neurologically induced, the ibogaine was discontinued, as was the amphetamine and Naprelan. About 24 hours after discontinuing the ibogaine, the client went into a 36 hour sleep and upon awakening, all involuntary movements had discontinued and normal gait and balance were restored. The patient had previously been on all the above mediations, except Naprelan, at various times over the past year, with no involuntary motor movements having been noted prior to the initiation of ibogaine.
These symptoms took some time to emerge (3-4 weeks) on the low dose of ibogaine (10-mg), suggesting that it was the gradually increasing levels of the nor-ibogaine metabolite that were likely the causal factor in interacting with the other medications. I remain uncertain as to what the causal factors were, or which of the medications were the likely candidates interacting with the ibogaine/nor-ibogaine to elicit this reaction (though I suspect the amphetamine). Anyone using small dosages of ibogaine to reduce tolerance should be mindful that interactions with other medications could result in unexpected reactions.
http://www.mindvox.com/pipermail/ibogaine/2007-July/031408.html
----
The effects herein described are those of single administration high dose ibogaine regimens. Ibogaine has also been given in regimens of small daily doses of 25 mg to 300 mgs/day and in small daily doses where the dose is increased on a daily basis until the desired interruption of drug dependence is accomplished. These low dose modalities have not been validated for efficacy to the same extent as have the full therapeutic doses of ibogaine. However, these low dose regimens can be traced back some decades to the work of Leo Zeff who in the case of a single patient provided ibogaine on an "as needed" basis via nasal administration to a cocaine dependent patient to substitute for his cocaine use. Lines of ibogaine were somewhat equivalent to lines of cocaine and the patient ceased cocaine use after a week of this daily self-regulated ibogaine regimen. Additionally, reports from Canadian sources indicate multi-week low dose ibogaine therapy 20 mg/day following a therapeutic dose of ibogaine in the treatment of cocaine dependence. Further, reports throughout the ibogaine provider community indicate the use of multiple dosing of varying strength doses over varying time periods in the treatment of opioid dependence. As with all determinations in medicine, decisions must be made on observations of the patient and knowledge of the disorder(s) and the medication(s) used.
https://truthtalk13.wordpress.com/2012/08/15/ibogaine-therapy/
-----
I started on a daily regime dose of 50mg of hcl 17 days ago. In the first 3-4 days my nicotine habit went down to nearly zero (it was an "effort" to smoke,if that makes any sense). In retrospect, I could have kicked with the minimum of effort, I didn't, which is more about my individual psychology/pathology than the efficiency of ibogaine in interrupting nicotine dependency. It seems that like high doses, a "window of opportunity" opens up and its up to the individual as always if they want to kick their chemical dependency. (After the 4th day, the effect seemed to diminish or at least get over written by continuing to smoke.)
HOWEVER!
My nicotine habit is at least 50% down daily as of today (from 12.5g of rolling tobacco to below 6.5g), and this is the first time I've ever tried to kick nicotine, apart from a few times in the cells where there wasn't much choice.
http://www.mindvox.com/pipermail/ibogaine/2003-April/004292.html
-----
Dr. Alper was among the attendees who gave a presentation on the benefits of ibogaine to the Catalan Ministry of Health. The prof believes ibogaine's most likely path to prominence in the United States will be as a medication for meth addiction, for the simple reason that doctors and treatment providers have found that small daily doses seem to work better for meth addiction than the mind-blowing "flood doses" used on opiate addicts. Alper says no one thought to try non-hallucinogenic quantities of ibogaine until recently. Ibogaine treatment providers tend to have been former ibogaine users, and most assumed that the introspection brought on by tripping was key to overcoming their addictions.
"That's just how it evolved," he says, noting that the large doses do seem to work best for opiate detox. "You're talking about a drug that has been used in less than 10,000 people in the world in terms of treatment. It's not surprising that's how it evolved. The visions have some psychological content that is salient and meaningful," Alper adds. "On the other hand, there is no successful treatment for addiction that's not interpreted as a spiritual transformation by the people who use it. It's the G-word. It's God. We as physicians don't venture into that territory, but most people do."
Recently Wilkins has been experimenting with small daily doses of ibogaine for people with heart conditions or other health problems that make the "flood dose" unadvisable. The non-hallucinogenic regimen seems successful, she says, citing the case of Ron Price, the former bodybuilder, in particular. Price first came to Tijuana for ibogaine in 1996 and has been back six times, including his October stay. "Every time I feel like I'm getting out of control, I come here," he says, his voice a gruff mumble. "The very first time, I had a bit of visuals. It's supposed to take six months to get off methadone. With this it was one day. It was incredible. I haven't had a craving for methadone since then." That first time, Price took a "flood dose," enough to keep him tripping for hours on end. During this stay, Wilkins started him off with a tiny dose and gradually increased the amount he ingested each day. At the same time, she was weaning him off Oxycontin.
"We reduced your Oxy dose from 240 milligrams to 120 milligrams, in what, two weeks? That's great!" she says encouragingly. "He was fantastic," she adds proudly. "He developed a routine in his day. He was getting up and watering the garden, and not staying in bed and watching TV. He was walking the dog and wanting to go out—he was eager to go home, not scared."
Now, seated at Pangea's kitchen table, Price reflects on what has been most helpful during his time in Mexico. The ibogaine lessened his cravings for drugs and alcohol, he says, but eventually the effect will wear off. "It's no magic thing," he says pensively. "It's creating good habits and creating a support system. Ibogaine just strips you of the cells and walls you build up for yourself. It allows you to go AA meetings—which I'll do when I get home. It at least gives you a fighting chance to make your own decision."
http://archive.seattleweekly.com/home/877106-129/story.html
----
Before dosing for long periods with iboga or using high doses for short periods, it is worth considering the potential damage it is doing to the Purkinje cells. The neurotoxicity appears to be species dependent and it really isn't known if it is a problem in primates . My gut instinct is in any case a low dose for longer periods of time is going to be safer than a high short term dose regime.
Ibogaine has also got some dangerous interactions with other drugs in particular opiates, which have killed people undergoing ibogaine therapy. FWIW there have been several deaths in treatment and the ibogaine clinics now screen out a lot of potential candidates. there appears to be some mechanism where it can cause heart arrhythmia and death. The pharmacology of ibogaine and the nor ibogaine metabolite is extremely dirty and complex.
IMHO the take home message is that ibogaine is fine if there is a purpose to using it ie quitting and therefore the risk benefit calculation works, because the risk associated with ibogaine is less than the risk of continued drug use, however taking ibogaine and continuing to use as well is just adding the risks of ibogaine but without removing the risk associated with continued drug use and therefore the risk benefit doesn't add up.
-vecktor
-----
It does have dangerous interactions with opiods - when used irresponsibly. What I wanted to relay, specifically, is that at LOW doses (again, 10 - 20mg) the opiate reset effect is fairly minimal - it seemed not so much to reset tolerance as to halt its development, which allowed me to use the chemicals I needed to in a stretch without incurring a massive habit, something that may be INCREDIBLY useful to people in chronic pain management situations. Now, I fully think that anyone taking it at all should probably have the arrhythmia screening - but then again, I also put up to your consideration the sale of lambarine, a 12mg ibogaine pep pill which was commonly sold in France at the turn of the century and seems to have no connotation of being dangerous or causing death in the people taking it. But vecktor overall is right - it is a risk calculation, in my particular situation it was "OMG, I'm doing some shit totally beyond the pall of normal human behavior, the end result of which may be completely unmanageable addiction and probably death, or I could try this untested compound in a new way that I have a hunch may just do the trick (I've done a flood dose before to kick dope)"
All I wanted to do is honestly relay that I feel this compound has saved my life a second time, and that continued low dose usage seems to have compounding positive effects both on my mental state and immune system. I don't know that I want to take it forever, it kind of seems to even mitigate administration of itself along with other chemicals, and as time goes on my drive to take it certainly diminishes. I'm not saying I want to take this stuff forever, I'm saying if I NEED it I never want to be without it I hope this reply clarifies some of my previous points, vecktor thank you for the voiced concern, I should have been more clear that P had already been screened for arrhythmia, and am familiar with ibo in general, if that wasn't the case id be much more concerned for my well being.
-cdin
-----
Here are excerpts taken from a journal of a friend of mine who used Low Dose Ibogaine and Memantine to overcome an opiate addiction and the terrible withdraws that come with it. I hope it helps others that are dealing with the horror of addiction and the hell of opiate withdraw. There is hope!
A quick background of my friend. I'll refer to him as "Bob".
Bob started an addiction to pain pills (vicoden, oxy, Opana) about 2 years ago. It went from a few vicodens a day and progressed to about 120-180 mgs of oxycodone per day. Bob got to the point of taking his last dose around 7:00 at night, then waking up around 2:30 in the morning in withdraws...cold sweats, restless legs and just that in ability to fall asleep without another fix. His motivation to work or get anything productive done was gone. His relationships suffered greatly and his life revolved around finding a way to get his next fix.
He thought about Suboxone treatment, but didn't want to trade one addiction for another. As many people know, coming off Suboxone is almost as painful as withdrawing from other opiates...something the Suboxone Doctors don't like to tell you.
This is when he started studying Ibogaine and Memantine. While Ibogaine is illegal in the USA and Memantine is very hard to get a prescription for, as most doctors have little sympathy for opiate addicts, especially when they aren't going to be making much money prescribing Memantine. They push suboxone because this ensures the doctor will keep you coming back and paying your hard earned money to them.
Both Ibogaine and Memantine can be found online, without a prescription, from reliable sources if you search hard enough. The Ibogaine used in Bob's experiment was the HCL form. It comes in 3 forms, HCL, TA and Root Bark. The best and most potent of the 3 is the HCL.
Bob started by cutting down his dose of oxy from 180 mgs to around 100 mgs per day. This was not enough to get him high, but enough to keep him out of withdraws.
Day 1: After receiving his Ibogaine and Memantine, he begain first thing in the morning, before taking any oxy, by taking a 5 mg of Memantine and about 30mgs of Ibogaine HCL on an empty stomach. This was to test and see if he had any allergies or adverse reactions to them. A slight stimulant effect was noticed from the Ibogaine and no real effect was noticed from the Memantine. 3 hours after, Bob took his usual doses of oxy throughout the day. No real changes where noticed.
•VERY IMPORTANT...be sure to wait at least three hours after taking Ibogaine before taking ANY opiate. Everyone is different and it's possible that the potentiating effects of Ibogaine could cause an overdose of whatever opiate you take. Until you know how this effects you, start with taking half of your usual opiate dose 3 hours after the Ibogaine and assess the results. Please be careful!
Day 2: Bob upped the dose of Ibogaine to 50 mgs first thing in the morning on an empty stomach. He also took 5 mgs of Memantine in the morning and another 5 in the evening. The Oxy was taken as usual.
This went on for 5 more days. Bob was still waking up in withdraws in the middle of the night for this first week but did notice they weren't nearly as bad.
Week 2:
Bob upped his dose to 100 mgs of Ibogaine first thing in the morning on an empty stomach along with the 5 mgs of Memantine in the morning and another 5 mgs in the evening. The Ibogaine definatly produced a stimulant effect and a very mild "Trippy" feeling that lasted about 2 hours. It was not uncomfortable and allowed Bob to still function normally.
By the end of the 2nd week, Bob was sleeping through the night with absolutely NO withdraw feelings waking him up. The Oxy was also slightly more potent. He also noticed that rather than having to take a morning dose of oxy, he could wait until around 2-3:00 in the afternoon before even the slightest feeling of withdraw would begin. This was amazing considering just 2 weeks earlier, Bob couldn't go more than 8-10 hours without having terrible withdraws. He was now able to go 17-20 hours before even the slightest withdraws started.
Week 3:
This week, Bob decided to take a larger dose of Ibogaine for 2 days in a row. He had off work on Monday and Tuesday so decided to take advantage of it.
Bob woke up on Monday and took 250 mgs of Ibogaine HCL with his normal 5 mg Memantine. This caused a bit more of a Trippy feeling that lasted about 3-5 hours. It wasn't uncomfortable,
just not something you should drive on at this dose. Memantine at 5 mgs was taken as usual that evening.
Tuesday Bob followed the same protocol as Monday.
By Wednesday, Bobs brain felt completely reset. The cravings for opiates were gone. He took 30 mgs of oxy Wednesday but just for fun...not out of a feeling of needing it or physical dependency.
Thursday, Bob continued to take Ibogaine but at a much lower dose...just 20 mgs first thing in the morning. He also took NO OPIATES AT ALL on this day. This is the first time in almost 2 years Bob as taken no opiate of any kind. He noticed slight chills that night but was able to fall back asleep with no real problem. He stopped all opiates for another 3 days just to be sure the the physical dependency was gone. I'm pleased to say it was. He had a fairly sever headache on day 2 but that was quickly remedied with 2 Excedrine Migraine pills.
Bob continued to take 20-50 mgs of Ibogaine and 5-10 mgs of Memantine for the next 2 weeks. He took an average of 1, 30mg oxycodone pill every other day. Each time was at a dose of 30 mgs of oxy. This was again, just for fun and not out of a feeling of physical dependency. I know you maybe asking why not just quit completely. According to Bob, he likes the ability to relax with an occasional opiate as opposed to a beer like most of us. Whether that's a good idea or not, at least it doesn't control his life anymore and he isn't physically dependent on opiates to function...each to his/her own I guess.
The strange thing was that while Bob's physical dependency for opiates was almost completely gone, he still required 30 mgs of oxycodone to get any kind of a high. One would expect tolerance to go down, requiring less oxy to get a buzz or get high. This was not the case with Bob but everyone is different.
In conclusion, it seems that their may be a way to completely avoid the horror of opiate withdraw, even with a fairly high tolerance and addiction. Everyone says that there's no magic bullet to cure withdraws...but after reading and seeing Bobs experience first hand, I would have to disagree. In just 5 weeks Bob went from a 2 year, 180 mg plus per day oxycodone addiction, down to absolutely no physical dependence at all. He did this with NO withdraws and even continued to take the occasional oxy for fun when we wanted.
Warning and disclaimer:
It would be irresponsible of me to suggest that this method of over coming opiate withdraw is for everyone. It's not. Before considering it, do your own research about the side effects of both Ibogaine and Memantine. Ibogaine should not be used by anyone with a pre-existing liver or heart problem. It should also not be taken in the evening as it is a stimulant. A thorough search of drug interactions, specifically with Memantine should also be done. Neither Bob nor myself are doctors so this information should NOT taken as medical advice.
I'd be happy to answer any questions as best I can. But to all those who are trapped in the hell of opiate addiction, there is hope. It's not cheap but it's certainly cheaper than a daily opiate addiction and much cheaper than any Suboxone treatment clinic.
I truly hope this helps someone. I saw it change my friend Bob's life first hand. I also believe it can be accomplished in less time than what it took Bob. If your motivated, I think one could over come opiate addiction with little to no withdraws in as little as 3 weeks.
If your willing to put yourself through a full flood dose of Ibogaine, one could even avoid opiate withdraw and overcome their physical addiction in 24-36 hours. This would not be what i would recommend however as the Flood Dose Trip can be VERY intense and possibly very dangerous. Unless you are in perfect medical condition AND have a care giver/babysitter to stay with you for the entire trip, I would strongly advise against it. I believe the low dose treatment option over a period of 2-5 weeks is the best and safest method to take.
It also must be noted that while Ibogaine and Memantine will get you through the physical addiction and withdraws fairly painlessly, the mental addiction will still be there. That said, it's very important to follow up with a support group of some kind...NA and/or AA meetings are very helpful and increase your chances of success in the long run greatly!
Having been through my own addictions and seen many others ruin their lives because of addiction, I understand the hell and shame of a downward spiral substance abuse can lead to. So when I find a method that works as well as the Low Dose Ibogaine/Memantine method, I get excited because I know it can change lives and heal those that are willing to be helped. Being a slave to a substance is no way to live and an easy way to die.
To all those that are struggling with opiate addiction...I'm here to tell you there's hope and a way to minimize if not completely eliminate the horrible opiate withdraws. All you need to do is decide to take that leap of faith! ;-)
Having gone through my own addiction issues and experienced the absolute hell of opiate withdraw on 3 separate occasions, (all were legally prescribed meds that I decided to quit on my own due to my inability to function at work while on pain meds) I have a great deal of compassion for anyone dealing with opiate addiction/withdraw.
There is no reason for anyone to go through the sleepless nights, vomiting, diarrhea and skin crawling joint pain of opiate withdraws ever again to get clean. There really is an alternative and I can't believe that in this country no one is using Ibogaine to get opiate addicts clean. It works and, while it isn't cheap, it's a hell of a lot cheaper than an opiate addiction. Not to mention it completely resets your brain and gives you back your motivation, and love for life again.
-workin2005
-----
Oxycodone habit aborted with low dose ibogaine
Fred had the rewarding opportunity to sit in on Josh's's detox from 150-180mg/day Oxy (insufflation) habit, duration of 3 months.
Subjects pre-history w/opiates:
*1999-2002 heroin habit 1-3gm/day (gaining daily intake by approximate 1gm per year, graduating from sniffing>smoking>shooting in the first year).
*late 2002 Successful Ibogaine hcl treatment.
*early 2010 Subject had surgery, resulting in Hydrocodone & Oxycodone habit, tapered down from 100mgs/day to 40mgs/day before a flood of Ibogaine hcl aprox 100 days after surgery, successful results.
*Mid 2012 subject injured neck in a bike wreck, resulting in the above mentioned recent habit (150-180mg/day Oxy)
Subject was gradually administered low doses of Iboga 80% TA (total alkaloid extract) in combination with small doses of methadone just prior to anticipated withdrawal symptoms. (Every 8-12 hours)
Subject metabolizes opiates quite rapidly, thus the methadone was administered in micro doses 2-3x/day. In combo of building up to a flood of the Iboga on day 3, as the Iboga was increased, the methadone was reduced by 1/3 (18-12-6-0), the 4th day being 0 opiates. Total Iboga amount required 470mg, spread across 5 days, with a peak of 200mg on day 3 (60-100-200-60-50).
Extreme care and calculations based on providers experience and open/honest dialogue and agreement with subject assured no risk of overdose, or an overwhelming Iboga experience, as the subject had already been through two single dose Ibogaine complete rebirths, with 12+hours of visuals and no sleep for 36 hours - which was quite overwhelming for the subject. This detox was more like an abortion as opposed to the classic Iboga rebirth.
The concept of introducing methadone in combo with the Iboga TA was two-fold:
1. To stabilize the subject from the ping-pong effect of short acting Oxy (going through withdrawals every 2-3 hours) while gently introducing the Iboga into the mix without a major Iboga experience.
2. Limited resources, Iboga is a precious sacred medicine!
Subject was able to sleep about 4-5 hours/night the first 2 nights with the administration of low doses of Valium, melatonin, L-Trytophan and 5-HTP. Sleep became an obstacle after the flood on day 3, getting only 2 hours of sleep, leaving subject a bit tattered on day 4, but hung in like a champ and got 4 hours sleep the following night.
Surprise surprise! During day 4 the subject was quite restless and was offered a small amount of cannabis (less than 1/20th/gm). This helped subject relax for a few minutes but then began to potentiate the Iboga (or vice-versa) and led to a 3 hour tearful cathartic experience - including visuals - illustrating the subject's traumas, failures, triumphs, lies, truths and challenges in life. Although subject was not comfortable with the process, literally 8-10 years peeled away from subject's face. As the processing subsided, subject was left with a deep calm, in spite of the challenges to be faced moving forward.
FYI, The cannabis was a Sativa variety - Dutch Treat. Had an Indica strain been available, the cannabis would have had a more sedating effect. It is Fred's opinion that Sativa varieties of cannabis have what Fred refers to as the truth serum effect, in addition to visualization, and psychoactive properties.
Subject is quite clear on day 5, was able to go food shopping and a short walk in nature, and has a complete 180 degree view on life and purpose moving forward. Aftercare plans include ending addictive associations of people, places and things and reaching out to Iboga peers met during previous treatments. Subject is not a 12 stepper, but does not rule out that in case of cravings, and is quite knowledgeable with the right supplements and physical activities for a healthy rebound.
Fred always finds it a blessing and miracle to witness a seemingly hopeless addict transform through the sacred medicine of Iboga. Aside from the spiritual/psychological healing aspects of Iboga are the physiological aspects of how the Ibogaine molecule helps reset/repair the opiate receptors/peptides.
-3rdStoneFromTheSun
BTW, I've been collecting reports about daily low dosing iboga (wonder if you might have an interest in that). Anyway, here are some (sorry to throw all this stuff at you willy-nilly):
Ibogaine has also been given in regimens of small daily doses of 25 to 300 mgs/day and in small daily doses where the dose is increased on a daily basis until the desired interruption of drug dependence is accomplished. These low dose modalities have not been validated for efficacy, however, they can be traced back some decades to the work of Leo Zeff who in the case of a single patient provided ibogaine on an "as needed" basis via nasal administration to a cocaine dependent patient to substitute for his cocaine use. Lines of ibogaine were somewhat equivalent to lines of cocaine, and the patient ceased cocaine use after a week of this daily self-regulated ibogaine regimen. Additionally, reports from Canadian sources indicate multi-week low dose ibogaine therapy 20 mg/day following a therapeutic dose of ibogaine in the treatment of cocaine dependence. Further, reports throughout the ibogaine provider community indicate the use of multiple dosing of varying strength doses over varying time periods in the treatment of opioid dependence. As with all determinations in medicine, decisions must be made based on observations of the patient and knowledge of the disorder(s) and the medication(s) used.
From the "Manual for Ibogaine Therapy Screening, Safety, Monitoring & Aftercare" by Howard S. Lotsof & Boaz Wachtel: http://ibogainedossier.com/manual.html
-----
There are 3 main options for ibogaine treatment (*these are all after a small test dose)
– single administration of 1 high dose ibogaine (with booster doses over the next few days/weeks if needed)
– single day/night of administration of multiple large doses spaced out by a few hours (with booster doses over the next few days/weeks as needed)
– small daily doses of 25-300 mg/day, where the dose is gradually increased each day until it is felt to have been effective for eliminating WDs/cravings (this one can be modified quite a bit)
http://www.dialogue.space/ibogaine-help-and-advice/
-----
Yes, small dosages are beneficial too, if one for example would like to deal just with the cravings. Not really sure though if Dr Mash`s theory of the effect of ibogaine metabolite (nor-ibogaine) staying long in the body really explains ibogaine`s long-term effects. It`s possible for example to take 200mg of Ibo HCl a week, or up to 50 mg a day...it`s very individual. Just don`t try the row powder from the iboga root - very harsh and very little effect.
http://archive.li/PMNzW
-----
My big bright idea, is to dose on opiates/opioids, and then take iboga root...but take a VERY small dose of iboga alkaloids, on a daily basis. and see if over time the iboga creates a potentiation of the opiate dose, allowing for reduction of the daily amount of opiates being used. I know one hypothesis is that the long lasting iboga metabolites cause part of the reduction/abolishment of opiate withdrawl...my idea hinges on this active metabolite hypothesis. The thought that a large, potentially dangerous, and mentally exhaustive standard iboga/ibogaine dose might be stretched out over a multitude of days and still create an active metabolite that has therapeutic value might appeal to people that are not ready for entry into a mindbending, physically taxing arena.
http://archive.li/PMNzW
-----
[Ibogaine] Ataxia and involuntary muscle movements induced by small daily doses interacting with other meds
I am posting this to the list in case anyone else may have had experience in this area and that hasn't posted it, and as an alert to others in case they see something like what I am about to describe develop. A client has been taking very small doses of ibogaine hcl (10-mg) once daily for approximately one month, to build up their nor-ibogaine levels so as to reduce tolerance to prescription pain medications. At the time the following symptoms emerged, the medication list included dilaudid (16mg q.i.d.), morphine sulfate (10mg as needed for breakthrough pain, about 3-4x daily), amphetamine (30-mg as needed to combat drowsiness of narcotics), Naprelan (Naprosyn extended release for mild arthritis), and Clonazepam (2-mg b.i.d.). A one-day trial of Trileptol (one dose) was initiated to possibly reduce the neuropathic pain being treated by the narcotics, but since this just made the client excessively sleepy it was not continued.
The client had not taken any amphetamine for approximately 2 weeks after initiating the ibogaine. About 4 days after initiating a small amount of amphetamine, the client developed involuntary muscle movements affecting the limbs and face. This included facial grimacing and eye rolling, as well as ataxia and loss of balance, including involuntary leg movements (bending at the knee and raising of the legs behind), arm movements, and sudden leg movements both forward and backwards. Since these movements were involuntary and obviously neurologically induced, the ibogaine was discontinued, as was the amphetamine and Naprelan. About 24 hours after discontinuing the ibogaine, the client went into a 36 hour sleep and upon awakening, all involuntary movements had discontinued and normal gait and balance were restored. The patient had previously been on all the above mediations, except Naprelan, at various times over the past year, with no involuntary motor movements having been noted prior to the initiation of ibogaine.
These symptoms took some time to emerge (3-4 weeks) on the low dose of ibogaine (10-mg), suggesting that it was the gradually increasing levels of the nor-ibogaine metabolite that were likely the causal factor in interacting with the other medications. I remain uncertain as to what the causal factors were, or which of the medications were the likely candidates interacting with the ibogaine/nor-ibogaine to elicit this reaction (though I suspect the amphetamine). Anyone using small dosages of ibogaine to reduce tolerance should be mindful that interactions with other medications could result in unexpected reactions.
http://www.mindvox.com/pipermail/ibogaine/2007-July/031408.html
----
The effects herein described are those of single administration high dose ibogaine regimens. Ibogaine has also been given in regimens of small daily doses of 25 mg to 300 mgs/day and in small daily doses where the dose is increased on a daily basis until the desired interruption of drug dependence is accomplished. These low dose modalities have not been validated for efficacy to the same extent as have the full therapeutic doses of ibogaine. However, these low dose regimens can be traced back some decades to the work of Leo Zeff who in the case of a single patient provided ibogaine on an "as needed" basis via nasal administration to a cocaine dependent patient to substitute for his cocaine use. Lines of ibogaine were somewhat equivalent to lines of cocaine and the patient ceased cocaine use after a week of this daily self-regulated ibogaine regimen. Additionally, reports from Canadian sources indicate multi-week low dose ibogaine therapy 20 mg/day following a therapeutic dose of ibogaine in the treatment of cocaine dependence. Further, reports throughout the ibogaine provider community indicate the use of multiple dosing of varying strength doses over varying time periods in the treatment of opioid dependence. As with all determinations in medicine, decisions must be made on observations of the patient and knowledge of the disorder(s) and the medication(s) used.
https://truthtalk13.wordpress.com/2012/08/15/ibogaine-therapy/
-----
I started on a daily regime dose of 50mg of hcl 17 days ago. In the first 3-4 days my nicotine habit went down to nearly zero (it was an "effort" to smoke,if that makes any sense). In retrospect, I could have kicked with the minimum of effort, I didn't, which is more about my individual psychology/pathology than the efficiency of ibogaine in interrupting nicotine dependency. It seems that like high doses, a "window of opportunity" opens up and its up to the individual as always if they want to kick their chemical dependency. (After the 4th day, the effect seemed to diminish or at least get over written by continuing to smoke.)
HOWEVER!
My nicotine habit is at least 50% down daily as of today (from 12.5g of rolling tobacco to below 6.5g), and this is the first time I've ever tried to kick nicotine, apart from a few times in the cells where there wasn't much choice.
http://www.mindvox.com/pipermail/ibogaine/2003-April/004292.html
-----
Dr. Alper was among the attendees who gave a presentation on the benefits of ibogaine to the Catalan Ministry of Health. The prof believes ibogaine's most likely path to prominence in the United States will be as a medication for meth addiction, for the simple reason that doctors and treatment providers have found that small daily doses seem to work better for meth addiction than the mind-blowing "flood doses" used on opiate addicts. Alper says no one thought to try non-hallucinogenic quantities of ibogaine until recently. Ibogaine treatment providers tend to have been former ibogaine users, and most assumed that the introspection brought on by tripping was key to overcoming their addictions.
"That's just how it evolved," he says, noting that the large doses do seem to work best for opiate detox. "You're talking about a drug that has been used in less than 10,000 people in the world in terms of treatment. It's not surprising that's how it evolved. The visions have some psychological content that is salient and meaningful," Alper adds. "On the other hand, there is no successful treatment for addiction that's not interpreted as a spiritual transformation by the people who use it. It's the G-word. It's God. We as physicians don't venture into that territory, but most people do."
Recently Wilkins has been experimenting with small daily doses of ibogaine for people with heart conditions or other health problems that make the "flood dose" unadvisable. The non-hallucinogenic regimen seems successful, she says, citing the case of Ron Price, the former bodybuilder, in particular. Price first came to Tijuana for ibogaine in 1996 and has been back six times, including his October stay. "Every time I feel like I'm getting out of control, I come here," he says, his voice a gruff mumble. "The very first time, I had a bit of visuals. It's supposed to take six months to get off methadone. With this it was one day. It was incredible. I haven't had a craving for methadone since then." That first time, Price took a "flood dose," enough to keep him tripping for hours on end. During this stay, Wilkins started him off with a tiny dose and gradually increased the amount he ingested each day. At the same time, she was weaning him off Oxycontin.
"We reduced your Oxy dose from 240 milligrams to 120 milligrams, in what, two weeks? That's great!" she says encouragingly. "He was fantastic," she adds proudly. "He developed a routine in his day. He was getting up and watering the garden, and not staying in bed and watching TV. He was walking the dog and wanting to go out—he was eager to go home, not scared."
Now, seated at Pangea's kitchen table, Price reflects on what has been most helpful during his time in Mexico. The ibogaine lessened his cravings for drugs and alcohol, he says, but eventually the effect will wear off. "It's no magic thing," he says pensively. "It's creating good habits and creating a support system. Ibogaine just strips you of the cells and walls you build up for yourself. It allows you to go AA meetings—which I'll do when I get home. It at least gives you a fighting chance to make your own decision."
http://archive.seattleweekly.com/home/877106-129/story.html
----
Before dosing for long periods with iboga or using high doses for short periods, it is worth considering the potential damage it is doing to the Purkinje cells. The neurotoxicity appears to be species dependent and it really isn't known if it is a problem in primates . My gut instinct is in any case a low dose for longer periods of time is going to be safer than a high short term dose regime.
Ibogaine has also got some dangerous interactions with other drugs in particular opiates, which have killed people undergoing ibogaine therapy. FWIW there have been several deaths in treatment and the ibogaine clinics now screen out a lot of potential candidates. there appears to be some mechanism where it can cause heart arrhythmia and death. The pharmacology of ibogaine and the nor ibogaine metabolite is extremely dirty and complex.
IMHO the take home message is that ibogaine is fine if there is a purpose to using it ie quitting and therefore the risk benefit calculation works, because the risk associated with ibogaine is less than the risk of continued drug use, however taking ibogaine and continuing to use as well is just adding the risks of ibogaine but without removing the risk associated with continued drug use and therefore the risk benefit doesn't add up.
-vecktor
-----
It does have dangerous interactions with opiods - when used irresponsibly. What I wanted to relay, specifically, is that at LOW doses (again, 10 - 20mg) the opiate reset effect is fairly minimal - it seemed not so much to reset tolerance as to halt its development, which allowed me to use the chemicals I needed to in a stretch without incurring a massive habit, something that may be INCREDIBLY useful to people in chronic pain management situations. Now, I fully think that anyone taking it at all should probably have the arrhythmia screening - but then again, I also put up to your consideration the sale of lambarine, a 12mg ibogaine pep pill which was commonly sold in France at the turn of the century and seems to have no connotation of being dangerous or causing death in the people taking it. But vecktor overall is right - it is a risk calculation, in my particular situation it was "OMG, I'm doing some shit totally beyond the pall of normal human behavior, the end result of which may be completely unmanageable addiction and probably death, or I could try this untested compound in a new way that I have a hunch may just do the trick (I've done a flood dose before to kick dope)"
All I wanted to do is honestly relay that I feel this compound has saved my life a second time, and that continued low dose usage seems to have compounding positive effects both on my mental state and immune system. I don't know that I want to take it forever, it kind of seems to even mitigate administration of itself along with other chemicals, and as time goes on my drive to take it certainly diminishes. I'm not saying I want to take this stuff forever, I'm saying if I NEED it I never want to be without it I hope this reply clarifies some of my previous points, vecktor thank you for the voiced concern, I should have been more clear that P had already been screened for arrhythmia, and am familiar with ibo in general, if that wasn't the case id be much more concerned for my well being.
-cdin
-----
Here are excerpts taken from a journal of a friend of mine who used Low Dose Ibogaine and Memantine to overcome an opiate addiction and the terrible withdraws that come with it. I hope it helps others that are dealing with the horror of addiction and the hell of opiate withdraw. There is hope!
A quick background of my friend. I'll refer to him as "Bob".
Bob started an addiction to pain pills (vicoden, oxy, Opana) about 2 years ago. It went from a few vicodens a day and progressed to about 120-180 mgs of oxycodone per day. Bob got to the point of taking his last dose around 7:00 at night, then waking up around 2:30 in the morning in withdraws...cold sweats, restless legs and just that in ability to fall asleep without another fix. His motivation to work or get anything productive done was gone. His relationships suffered greatly and his life revolved around finding a way to get his next fix.
He thought about Suboxone treatment, but didn't want to trade one addiction for another. As many people know, coming off Suboxone is almost as painful as withdrawing from other opiates...something the Suboxone Doctors don't like to tell you.
This is when he started studying Ibogaine and Memantine. While Ibogaine is illegal in the USA and Memantine is very hard to get a prescription for, as most doctors have little sympathy for opiate addicts, especially when they aren't going to be making much money prescribing Memantine. They push suboxone because this ensures the doctor will keep you coming back and paying your hard earned money to them.
Both Ibogaine and Memantine can be found online, without a prescription, from reliable sources if you search hard enough. The Ibogaine used in Bob's experiment was the HCL form. It comes in 3 forms, HCL, TA and Root Bark. The best and most potent of the 3 is the HCL.
Bob started by cutting down his dose of oxy from 180 mgs to around 100 mgs per day. This was not enough to get him high, but enough to keep him out of withdraws.
Day 1: After receiving his Ibogaine and Memantine, he begain first thing in the morning, before taking any oxy, by taking a 5 mg of Memantine and about 30mgs of Ibogaine HCL on an empty stomach. This was to test and see if he had any allergies or adverse reactions to them. A slight stimulant effect was noticed from the Ibogaine and no real effect was noticed from the Memantine. 3 hours after, Bob took his usual doses of oxy throughout the day. No real changes where noticed.
•VERY IMPORTANT...be sure to wait at least three hours after taking Ibogaine before taking ANY opiate. Everyone is different and it's possible that the potentiating effects of Ibogaine could cause an overdose of whatever opiate you take. Until you know how this effects you, start with taking half of your usual opiate dose 3 hours after the Ibogaine and assess the results. Please be careful!
Day 2: Bob upped the dose of Ibogaine to 50 mgs first thing in the morning on an empty stomach. He also took 5 mgs of Memantine in the morning and another 5 in the evening. The Oxy was taken as usual.
This went on for 5 more days. Bob was still waking up in withdraws in the middle of the night for this first week but did notice they weren't nearly as bad.
Week 2:
Bob upped his dose to 100 mgs of Ibogaine first thing in the morning on an empty stomach along with the 5 mgs of Memantine in the morning and another 5 mgs in the evening. The Ibogaine definatly produced a stimulant effect and a very mild "Trippy" feeling that lasted about 2 hours. It was not uncomfortable and allowed Bob to still function normally.
By the end of the 2nd week, Bob was sleeping through the night with absolutely NO withdraw feelings waking him up. The Oxy was also slightly more potent. He also noticed that rather than having to take a morning dose of oxy, he could wait until around 2-3:00 in the afternoon before even the slightest feeling of withdraw would begin. This was amazing considering just 2 weeks earlier, Bob couldn't go more than 8-10 hours without having terrible withdraws. He was now able to go 17-20 hours before even the slightest withdraws started.
Week 3:
This week, Bob decided to take a larger dose of Ibogaine for 2 days in a row. He had off work on Monday and Tuesday so decided to take advantage of it.
Bob woke up on Monday and took 250 mgs of Ibogaine HCL with his normal 5 mg Memantine. This caused a bit more of a Trippy feeling that lasted about 3-5 hours. It wasn't uncomfortable,
just not something you should drive on at this dose. Memantine at 5 mgs was taken as usual that evening.
Tuesday Bob followed the same protocol as Monday.
By Wednesday, Bobs brain felt completely reset. The cravings for opiates were gone. He took 30 mgs of oxy Wednesday but just for fun...not out of a feeling of needing it or physical dependency.
Thursday, Bob continued to take Ibogaine but at a much lower dose...just 20 mgs first thing in the morning. He also took NO OPIATES AT ALL on this day. This is the first time in almost 2 years Bob as taken no opiate of any kind. He noticed slight chills that night but was able to fall back asleep with no real problem. He stopped all opiates for another 3 days just to be sure the the physical dependency was gone. I'm pleased to say it was. He had a fairly sever headache on day 2 but that was quickly remedied with 2 Excedrine Migraine pills.
Bob continued to take 20-50 mgs of Ibogaine and 5-10 mgs of Memantine for the next 2 weeks. He took an average of 1, 30mg oxycodone pill every other day. Each time was at a dose of 30 mgs of oxy. This was again, just for fun and not out of a feeling of physical dependency. I know you maybe asking why not just quit completely. According to Bob, he likes the ability to relax with an occasional opiate as opposed to a beer like most of us. Whether that's a good idea or not, at least it doesn't control his life anymore and he isn't physically dependent on opiates to function...each to his/her own I guess.
The strange thing was that while Bob's physical dependency for opiates was almost completely gone, he still required 30 mgs of oxycodone to get any kind of a high. One would expect tolerance to go down, requiring less oxy to get a buzz or get high. This was not the case with Bob but everyone is different.
In conclusion, it seems that their may be a way to completely avoid the horror of opiate withdraw, even with a fairly high tolerance and addiction. Everyone says that there's no magic bullet to cure withdraws...but after reading and seeing Bobs experience first hand, I would have to disagree. In just 5 weeks Bob went from a 2 year, 180 mg plus per day oxycodone addiction, down to absolutely no physical dependence at all. He did this with NO withdraws and even continued to take the occasional oxy for fun when we wanted.
Warning and disclaimer:
It would be irresponsible of me to suggest that this method of over coming opiate withdraw is for everyone. It's not. Before considering it, do your own research about the side effects of both Ibogaine and Memantine. Ibogaine should not be used by anyone with a pre-existing liver or heart problem. It should also not be taken in the evening as it is a stimulant. A thorough search of drug interactions, specifically with Memantine should also be done. Neither Bob nor myself are doctors so this information should NOT taken as medical advice.
I'd be happy to answer any questions as best I can. But to all those who are trapped in the hell of opiate addiction, there is hope. It's not cheap but it's certainly cheaper than a daily opiate addiction and much cheaper than any Suboxone treatment clinic.
I truly hope this helps someone. I saw it change my friend Bob's life first hand. I also believe it can be accomplished in less time than what it took Bob. If your motivated, I think one could over come opiate addiction with little to no withdraws in as little as 3 weeks.
If your willing to put yourself through a full flood dose of Ibogaine, one could even avoid opiate withdraw and overcome their physical addiction in 24-36 hours. This would not be what i would recommend however as the Flood Dose Trip can be VERY intense and possibly very dangerous. Unless you are in perfect medical condition AND have a care giver/babysitter to stay with you for the entire trip, I would strongly advise against it. I believe the low dose treatment option over a period of 2-5 weeks is the best and safest method to take.
It also must be noted that while Ibogaine and Memantine will get you through the physical addiction and withdraws fairly painlessly, the mental addiction will still be there. That said, it's very important to follow up with a support group of some kind...NA and/or AA meetings are very helpful and increase your chances of success in the long run greatly!
Having been through my own addictions and seen many others ruin their lives because of addiction, I understand the hell and shame of a downward spiral substance abuse can lead to. So when I find a method that works as well as the Low Dose Ibogaine/Memantine method, I get excited because I know it can change lives and heal those that are willing to be helped. Being a slave to a substance is no way to live and an easy way to die.
To all those that are struggling with opiate addiction...I'm here to tell you there's hope and a way to minimize if not completely eliminate the horrible opiate withdraws. All you need to do is decide to take that leap of faith! ;-)
Having gone through my own addiction issues and experienced the absolute hell of opiate withdraw on 3 separate occasions, (all were legally prescribed meds that I decided to quit on my own due to my inability to function at work while on pain meds) I have a great deal of compassion for anyone dealing with opiate addiction/withdraw.
There is no reason for anyone to go through the sleepless nights, vomiting, diarrhea and skin crawling joint pain of opiate withdraws ever again to get clean. There really is an alternative and I can't believe that in this country no one is using Ibogaine to get opiate addicts clean. It works and, while it isn't cheap, it's a hell of a lot cheaper than an opiate addiction. Not to mention it completely resets your brain and gives you back your motivation, and love for life again.
-workin2005
-----
Oxycodone habit aborted with low dose ibogaine
Fred had the rewarding opportunity to sit in on Josh's's detox from 150-180mg/day Oxy (insufflation) habit, duration of 3 months.
Subjects pre-history w/opiates:
*1999-2002 heroin habit 1-3gm/day (gaining daily intake by approximate 1gm per year, graduating from sniffing>smoking>shooting in the first year).
*late 2002 Successful Ibogaine hcl treatment.
*early 2010 Subject had surgery, resulting in Hydrocodone & Oxycodone habit, tapered down from 100mgs/day to 40mgs/day before a flood of Ibogaine hcl aprox 100 days after surgery, successful results.
*Mid 2012 subject injured neck in a bike wreck, resulting in the above mentioned recent habit (150-180mg/day Oxy)
Subject was gradually administered low doses of Iboga 80% TA (total alkaloid extract) in combination with small doses of methadone just prior to anticipated withdrawal symptoms. (Every 8-12 hours)
Subject metabolizes opiates quite rapidly, thus the methadone was administered in micro doses 2-3x/day. In combo of building up to a flood of the Iboga on day 3, as the Iboga was increased, the methadone was reduced by 1/3 (18-12-6-0), the 4th day being 0 opiates. Total Iboga amount required 470mg, spread across 5 days, with a peak of 200mg on day 3 (60-100-200-60-50).
Extreme care and calculations based on providers experience and open/honest dialogue and agreement with subject assured no risk of overdose, or an overwhelming Iboga experience, as the subject had already been through two single dose Ibogaine complete rebirths, with 12+hours of visuals and no sleep for 36 hours - which was quite overwhelming for the subject. This detox was more like an abortion as opposed to the classic Iboga rebirth.
The concept of introducing methadone in combo with the Iboga TA was two-fold:
1. To stabilize the subject from the ping-pong effect of short acting Oxy (going through withdrawals every 2-3 hours) while gently introducing the Iboga into the mix without a major Iboga experience.
2. Limited resources, Iboga is a precious sacred medicine!
Subject was able to sleep about 4-5 hours/night the first 2 nights with the administration of low doses of Valium, melatonin, L-Trytophan and 5-HTP. Sleep became an obstacle after the flood on day 3, getting only 2 hours of sleep, leaving subject a bit tattered on day 4, but hung in like a champ and got 4 hours sleep the following night.
Surprise surprise! During day 4 the subject was quite restless and was offered a small amount of cannabis (less than 1/20th/gm). This helped subject relax for a few minutes but then began to potentiate the Iboga (or vice-versa) and led to a 3 hour tearful cathartic experience - including visuals - illustrating the subject's traumas, failures, triumphs, lies, truths and challenges in life. Although subject was not comfortable with the process, literally 8-10 years peeled away from subject's face. As the processing subsided, subject was left with a deep calm, in spite of the challenges to be faced moving forward.
FYI, The cannabis was a Sativa variety - Dutch Treat. Had an Indica strain been available, the cannabis would have had a more sedating effect. It is Fred's opinion that Sativa varieties of cannabis have what Fred refers to as the truth serum effect, in addition to visualization, and psychoactive properties.
Subject is quite clear on day 5, was able to go food shopping and a short walk in nature, and has a complete 180 degree view on life and purpose moving forward. Aftercare plans include ending addictive associations of people, places and things and reaching out to Iboga peers met during previous treatments. Subject is not a 12 stepper, but does not rule out that in case of cravings, and is quite knowledgeable with the right supplements and physical activities for a healthy rebound.
Fred always finds it a blessing and miracle to witness a seemingly hopeless addict transform through the sacred medicine of Iboga. Aside from the spiritual/psychological healing aspects of Iboga are the physiological aspects of how the Ibogaine molecule helps reset/repair the opiate receptors/peptides.
-3rdStoneFromTheSun
Last edited:
- Joined
- Jul 2, 2008
- Messages
- 9,131
Form what I've read (and I didn't read all the posts here), Ibogaine is mostly neurotoxic, causing some kind of tremors/seizure.
^ No, not really.. the studies (actually one) of Ibogaine neurotoxicity (part of a studies of NMDA antagonists neurotoxicty in general) used humongous doses in rats (something like equivalent to 10-15 g in humans!!) to show lesions in Purkinje cells in rats cerebellum. This is like 10x flood doses of Ibogaine used for PAWS and opiates cravings. (I'll post the study later when time permits..). Tremors and ataxia at flood doses yeah but i never heard about Ibogaine causing seizures!!
^^ nice jobs summarizing that study out of Austria.. ( I think there are more papers from Pr Koenig group on Ibogaine and hERG.. will post more later time permitting)..
As for microdosing, yeah I think it is the way to go. Microdosing Iboga has tremendous potential especially for heavy depression and anxiety. Maybe even more useful than for OP treatment. Ibogaine is pretty safe at low doses (a NIH/FDA phase 1 clinical trial in 1990s evaluating 300mg dose in healthy volunteers showed it is well tolerated with no obvious side-effects including cardiovascular at this dose. But that was right before NIH helped scheduled Ibogaine and 'killed" all future clinical studies of Ibogaine in the US.
Anyhow, it does truly "magic" for depression, anxiety, PTSD and other moods problems. Most of the time, Ibogaine is mostly known for opiates withdrawals but the Plant has amazing effect on treating heavy depression .. here is a remarkable story: (don't miss the whole video..watch the whole thing if you can .. It is quite amazing how the molecule bring back from deepest darkness of heavy depression..
Microdosing Ibogaine for heavy depression:
[video]https://youtu.be/JZcm_ayPi3Y[/video]
^^ nice jobs summarizing that study out of Austria.. ( I think there are more papers from Pr Koenig group on Ibogaine and hERG.. will post more later time permitting)..
As for microdosing, yeah I think it is the way to go. Microdosing Iboga has tremendous potential especially for heavy depression and anxiety. Maybe even more useful than for OP treatment. Ibogaine is pretty safe at low doses (a NIH/FDA phase 1 clinical trial in 1990s evaluating 300mg dose in healthy volunteers showed it is well tolerated with no obvious side-effects including cardiovascular at this dose. But that was right before NIH helped scheduled Ibogaine and 'killed" all future clinical studies of Ibogaine in the US.
Anyhow, it does truly "magic" for depression, anxiety, PTSD and other moods problems. Most of the time, Ibogaine is mostly known for opiates withdrawals but the Plant has amazing effect on treating heavy depression .. here is a remarkable story: (don't miss the whole video..watch the whole thing if you can .. It is quite amazing how the molecule bring back from deepest darkness of heavy depression..
Microdosing Ibogaine for heavy depression:
[video]https://youtu.be/JZcm_ayPi3Y[/video]
mr peabody
Bluelight Crew
- Joined
- Aug 31, 2016
- Messages
- 5,714
( I think there are more papers from Pr Koenig group on Ibogaine and hERG.. will post more later time permitting)..
Must have those papers!
ok! I'll watch it!Anyhow, it does truly "magic" for depression, anxiety, PTSD and other moods problems. Most of the time, Ibogaine is mostly known for opiates withdrawals but the Plant has amazing effect on treating heavy depression .. here is a remarkable story: (don't miss the whole video..watch the whole thing if you can .. It is quite amazing how the molecule bring back from deepest darkness of heavy depression..
Microdosing Ibogaine for heavy depression:
[video]https://youtu.be/JZcm_ayPi3Y[/video]
Meanwhile, I've just run across this:
18-Methylaminocoronaridine (18-MAC)
(–)-18-Methylaminocoronaridine (18-MAC) is a second generation synthetic derivative of ibogaine developed by the research team led by Stanley Glick and Martin Kuehne. In animal studies it has shown around twice the efficacy of the related compound 18-methoxycoronaridine (18-MC) at reducing self-administration of morphine when administered in an equivalent dose, although less effective than 18-MC at reducing methamphetamine administration. Like 18-MC, 18-MAC acts primarily as a selective α3β4 nicotinic acetylcholine antagonist, and is even more selective than 18-MC with very little activity as an NMDA antagonist and only slight affinity for the delta opioid receptor.
https://en.wikipedia.org/wiki/18-Methylaminocoronaridine
-----

18-Methoxycoronaridine (18-MC)*
Dr. Stanley Glick spent much of his career exploring ibogaine, in partnership with Dr. Martin Kuehne. Glick thought ibogaine had a lot of promise if he could somehow fix its side effects.
"Kuehne began sending me one derivative of ibogaine after another. We eventually tested about 60 of them, but it was about the 15th compound that we found what we were looking for. Meaning that we found a drug that seemed to produce all the positive putative effects of ibogaine. It worked in all of the addiction models in the laboratory similar to the way ibogaine had worked, but it lacked all the toxicity. We found a drug that seems to produce all the positive putative effects of ibogaine, that works in all of the addiction models in the laboratory similar to the way ibogaine works, but it lacks all the toxicity. It's called 18-Methoxycoronaridine, or 18-MC for short."
So it was that Glick and Kuehne discovered 18-MC, which Glick does not believe will cause hallucinations, around 1995. Glick had some false starts finding a company to develop the drug, but eventually hooked up with Savant HWP Inc. of San Carlos, California, just south of San Francisco.
Glick says he hopes to see 18-MC approved in his lifetime. Even now, he says, he regularly takes calls from desperate heroin addicts or their parents hoping to get the drug.
"It's always depressing," he says, "because I can't give them any help right now."
Stephen Hurst, president and CEO of Savant HWP, explains 18-MC this way.
"Organic molecules have what's known as a backbone structure, a skeletal structure, and it can be a carbon chain, a circle of carbon atoms ... so ibogaine and 18-MC share the same chemical backbone," he says.
"Glick and Kuehne," he says, "changed the "side chains," the molecules that hang off of the backbone. Then 18-MC proved to be the side chain change that had the desired effect, anti-addictive qualities, minus the psychedelic effects and toxicity."
Hurst calls 18-MC an extremely exciting drug, because it does something that no other addiction drug has ever done.
"Addictions can come from different areas," he explains. "Cocaine works in a different way than heroin works. Nicotine works in a different way than heroin and cocaine. Methamphetamine works differently. Alcohol works differently. But they all have the same result, which is ... they all result in a storm of dopamine in the reward centers of the brain, which has neurons that project into the frontal cortex."
"So you actually have the precept of pleasure as a result of these compounds. And I mean, we all know, pleasurable experiences are very compelling. They're sure a lot more compelling than unpleasurable ones. The brain learns to seek out these compounds, these substances, or engage in these behaviors that cause this dopamine storm, if you will. And that becomes associated with environmental cues. What the brain will do is if you give it an environmental cue, it will already start to up-regulate the dopamine, but then if you don't get the substance, the brain kind of shuts everything down and withdraws dopamine back into the neurons in the pleasure centers of the brain. And that causes extreme distress."
"That's what craving is caused by. That's what causes recidivism and alcoholism and smoking and opiate, any form of addiction. As I describe it, it's why I can go into a Starbucks with the best of intentions of coming out with a tea and a banana, and end up walking out of the door with three bites out of a scone."
So here's what makes 18-MC different, Hurst says:
"This is the first drug that there is conclusive research data that show that it's effective regardless of what the substance is, which means the drug is working at the central mechanism of the disease, which is dopamine disregulation in the reward centers in the mid-brain. ... This is the same part of the brain that our fight or flight mechanism comes from, it's very primitive. It's common in all mammals and all substances, and certain compulsive behaviors as well. Basically they start off at different ends of town, but they all end up in the town square, which is dopamine disregulation. And this is the first drug that seems to reverse that dopamine disregulation in the reward centers of the brain."
Hurst says that so far, it appears that 18-MC is what it promised to be. The first round of testing in rats showed no cardiovascular or psychedelic effects, but it appears comparable to ibogaine in fighting addiction.
"Additionally, we've done the initial human testing, which for this drug was a very important risk reduction point, because if we gave it to people and they started hallucinating, it would have been a nonstarter. We didn't see any signs of that kind of behavior in nonhuman primate studies that we did, but there's always a chance that a human being is going to deal with a drug very differently than a nonhuman primate or a rat or a dog, and we had to make sure we did not have that problem. This is the first drug that seems to reverse that dopamine disregulation in the reward centers of the brain."
The company is planning two years of testing on healthy humans, and then addicts, for starters. Those initial tests will likely look at issues like how the drug affects people with food in their stomach, if the effect is different depending on gender, which dosage level is optimal and whether tobacco interacts with the drug.
It's still early in the process for 18-MC, which is in the first phase of Food and Drug Administration testing. Generally, three phases are required, though sometimes drugs are allowed to go onto the market after 2. Other times it takes 4. When a drug is considered safe enough to go to market, it's examined by an expert committee, which makes a recommendation to the commissioner, who ultimately decides its fate.
Hurst says his company generally takes drugs through the first two phases of development independently, at a cost of $25 million to $50 million for a drug like 18-MC. When the drug reaches Phase 3, the company tries to partner with a multinational pharmaceutical company to help foot the bill for the most expensive tests.
All of this means that getting 18-MC to the market could take anywhere from two to five years, if everything goes well.
"We're very optimistic about this drug," he says, "but we're still very early in the human testing."
Interestingly, 18-MC also appears to work against a parasitic disease called Leishmaniasis, common in many countries including Brazil and Afghanistan. Millions of patients are affected by the disease, which comes in three forms that can cause everything from disfiguring lesions, to death, to the inability to eat. While it's treatable, 18-MC has the potential to treat the disease in a simpler fashion than is now available, with a pill.
Hurst says he's not positive what addictions 18-MC might be developed to treat. Since testing is so expensive, it will likely be targeted toward only some of the things it has the potential to treat. That could be heroin or nicotine addiction, or Leishmaniasis. Some of the considerations include what is easiest to get through the FDA. But it also matters what the company can get funding to test.
For some, the development of 18-MC may be a disappointment. Addicts who have used ibogaine often say the hallucinations are a huge part of the healing experience, that they lead them through a re-examination of their lives and endow them with wisdom. But 18-MC wouldn't do that.
Still, with its ability to halt withdrawals, 18-MC has the potential to be the best treatment for serious drug addiction. Yet it may be hard to predict just how effective it would be. First, there isn't exactly an official tracking system to measure ibogaine's effectiveness. Second, even with traditional methods, addiction recovery rates aren't straightforward.
That fact was noted in a Pulitzer Prize-nominated, 8-part series on a maintenance drug for opioid addicts called Suboxone, similar to the more commonly known Methadone. The series, called "Dying to be free," outlines the struggle of addicts to get access to Suboxone, which for many is more effective than 12-step programs.
And when it comes to 18-MC, those statistics become trickier, as it's hard to define what ibogaine actually is. Doug Greene, GITA's patient advocacy coordinator at the nonprofit's Montreal headquarters, says in an interview that it's important to remember ibogaine doesn't cure heroin addiction. It simply gives users a better chance, because it halts withdrawals and, through hallucinations, provides insights into one's life.
"But once it's administered, patients should seek other treatments, including therapy. In some cases," Greene says, "patients may even benefit from going on a maintenance drug like Suboxone or Methadone after ibogaine treatment. Ibogaine is an amazing, incredibly valuable tool to help people get into recovery," said Greene.
*From the article here: https://www.csindy.com/coloradosprin...nt?oid=3927464
Last edited:
Form what I've read (and I didn't read all the posts here), Ibogaine is mostly neurotoxic, causing some kind of tremors/seizure.
It causes ataxia, which manifests as a constant shaking, vibration, or as you put it tremors; I have experienced this firsthand, it doesn't feel seizure related, and I doubt it has anything to do with neurotoxicity or lack thereof and only seems tangentially related to any of its other effects. Unless you are talking about something else.
^ Yeah right the ataxia and tremors are not centrally mediated ie have nothing to do with Iboga action in the brain but rather its neuromuscular actions. This is due to Ibogaine and related iboga compounds having cholinergic blocking activity: keeping in mind these happen only in flood doses, nothing to worry about imho : laying down and avoid moving around after flood dose solve the problem which usually last 2-3 hours.. The most serious issues with Ibogaine tho is 1. vomiting so one doesn't really know whether the intended dose is fully absorbed or not and 2. cardiotoxicity ( here is a old thread on this : hERG channel blockade and prolonged QT interval from iboga alkaloids )
^^ Nice overview of Stan Glick work on MC-18 and related iboga compounds .. few comments:
Compare the chemical structures of Ibogaine, Voacangine, 18-MC and Coronaridine:
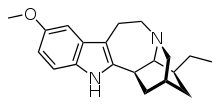
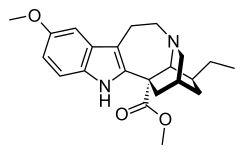
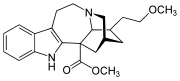
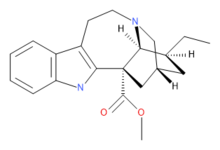
first structure is Ibogaine then Voacangine then 18-MC then Coronaridine
Now, one of the problem with coronaridine alkaloids is they induce seizure at large doses (at least Voacangine does .. ). Considering the close similarity between Voacangine and 18-MC one would expect 18-MC to aslo induce seizure at large doses. But we don't know for sure since afaik no study reported using large doses of 18-MC.. so who knows?.
Another interesting issues with 18-MC, is that reportedly it does not induce "hallucinations" more correctly "visions" since it is not really correct to describe Iboga visions as "hallucinations" but more like recollection (ie memory retrieval either emotionally charged or not.. here is a study: Facilitation of memory retrieval by the "anti-addictive" alkaloid, ibogaine. ). The problem is: the "visions" ARE THE CURE.. imho. Ibogaine "visions" are required for long term cessation of craving at least with opiates (90% of people who benefit long term cessation of craving reported the visions and psychological introspection experienced during Ibogaine experience as the key factor that help them stay sober long term..) Of course this is in addition to Iboagaine effects in treating withdrawals acutely.
So the issue wth Stan Glick 18-MC is that if they dont induce "Hallucinations" Visions..etc would they be like Ibogaine in term of cessation of long term cravings ..who knows? And that's in addition to the cardiovascular issue common to both Ibogaine and 18MC, Voacangine.. which is why I said earlier I see no benefits of these compared to plain Iboga Total Alkaloid (ITA) extracts or IbogaineHCL.
On the other hand, synthetic derivatives of Ibogaine with NO CARDIOVASCULAR SIDE-EFFECTS like those claimed by that Canadian biotek company would make a billion dollar drug. why? because the single biggest obstacle to widespread use of Ibogaine imho is the heart issue. before treatment, people have to be first screened for heart diseases/conditions..etc and then treated in clinics which most people can't afford. So if you have a safe and effective Ibogaine analogs that people can use without the need for heart screening and clinics, I mean something people can use safely at home, then you probably have a billion dollar compounds. By safe, I mean to say like as safe as a cannabis joint..
Anyway, should anybody come across chemical structures of those compounds (non-cardiotoxic Iboagine congeners).. thx4posting
^^ Nice overview of Stan Glick work on MC-18 and related iboga compounds .. few comments:
yes and no!.. technically 18-MC, 18-MAC and related compounds are derivatives of VOACANGINE or CORONARIDINE not IBOGAINE although it is true Voacangine is related to Ibogaine but those two have rather different pharmacology:(–)-18-Methylaminocoronaridine (18-MAC) is a second generation synthetic derivative of ibogaine
Compare the chemical structures of Ibogaine, Voacangine, 18-MC and Coronaridine:
first structure is Ibogaine then Voacangine then 18-MC then Coronaridine
Now, one of the problem with coronaridine alkaloids is they induce seizure at large doses (at least Voacangine does .. ). Considering the close similarity between Voacangine and 18-MC one would expect 18-MC to aslo induce seizure at large doses. But we don't know for sure since afaik no study reported using large doses of 18-MC.. so who knows?.
Another interesting issues with 18-MC, is that reportedly it does not induce "hallucinations" more correctly "visions" since it is not really correct to describe Iboga visions as "hallucinations" but more like recollection (ie memory retrieval either emotionally charged or not.. here is a study: Facilitation of memory retrieval by the "anti-addictive" alkaloid, ibogaine. ). The problem is: the "visions" ARE THE CURE.. imho. Ibogaine "visions" are required for long term cessation of craving at least with opiates (90% of people who benefit long term cessation of craving reported the visions and psychological introspection experienced during Ibogaine experience as the key factor that help them stay sober long term..) Of course this is in addition to Iboagaine effects in treating withdrawals acutely.
So the issue wth Stan Glick 18-MC is that if they dont induce "Hallucinations" Visions..etc would they be like Ibogaine in term of cessation of long term cravings ..who knows? And that's in addition to the cardiovascular issue common to both Ibogaine and 18MC, Voacangine.. which is why I said earlier I see no benefits of these compared to plain Iboga Total Alkaloid (ITA) extracts or IbogaineHCL.
On the other hand, synthetic derivatives of Ibogaine with NO CARDIOVASCULAR SIDE-EFFECTS like those claimed by that Canadian biotek company would make a billion dollar drug. why? because the single biggest obstacle to widespread use of Ibogaine imho is the heart issue. before treatment, people have to be first screened for heart diseases/conditions..etc and then treated in clinics which most people can't afford. So if you have a safe and effective Ibogaine analogs that people can use without the need for heart screening and clinics, I mean something people can use safely at home, then you probably have a billion dollar compounds. By safe, I mean to say like as safe as a cannabis joint..
Anyway, should anybody come across chemical structures of those compounds (non-cardiotoxic Iboagine congeners).. thx4posting
Last edited:
mr peabody
Bluelight Crew
- Joined
- Aug 31, 2016
- Messages
- 5,714
^ Wonderful. May I have your permission to re-post that here (bottom): http://www.bluelight.org/vb/threads/823455-Ibogaine-and-opiate-opioid-addiction
^ Fascinating. And thanks for the link to Facilitation of memory retrieval by the "anti-addictive" alkaloid, ibogaine. Do you have the complete paper?
A few more bits...
A number of derivatives of 18-MC have also been developed, with several being superior to 18-MC itself, the methoxyethyl congener ME-18-MC being more potent than 18-MC but with similar efficacy.
(–)-2-Methoxyethyl-18-methoxycoronaridinate (ME-18-MC) is a second generation synthetic derivative of ibogaine developed by Glick and Kuehne. In animal studies it has shown similar efficacy to 18-MC at reducing self-administration of morphine and methamphetamine but with higher potency by weight, showing anti-addictive effects at the equivalent of half the minimum effective dose of 18-MC. Similarly to 18-MC itself, ME-18-MC acts primarily as a selective αβ nicotinic acetylcholine antagonist, although it has a slightly stronger effect than 18-MC as an NMDA antagonist, and its effects on opioid receptors are weaker than those of 18-MC at all except the kappa opioid receptor, at which it has slightly higher affinity than 18-MC.
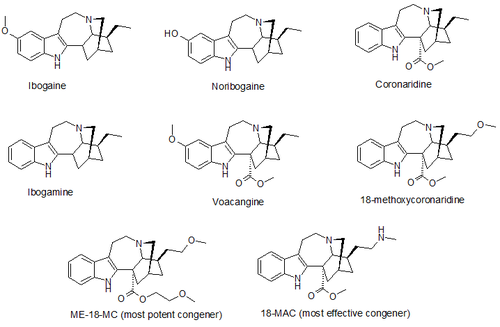
I find three 2nd generation congeners: 18-MC, 18-MAC and ME-18-MC. Is that all of these?
Are you set up to develop an analog that people can use safely at home? If so, I'd like to help.
( here is a old thread on this : hERG channel blockade and prolonged QT interval from iboga alkaloids )
^ Fascinating. And thanks for the link to Facilitation of memory retrieval by the "anti-addictive" alkaloid, ibogaine. Do you have the complete paper?
A few more bits...
A number of derivatives of 18-MC have also been developed, with several being superior to 18-MC itself, the methoxyethyl congener ME-18-MC being more potent than 18-MC but with similar efficacy.
(–)-2-Methoxyethyl-18-methoxycoronaridinate (ME-18-MC) is a second generation synthetic derivative of ibogaine developed by Glick and Kuehne. In animal studies it has shown similar efficacy to 18-MC at reducing self-administration of morphine and methamphetamine but with higher potency by weight, showing anti-addictive effects at the equivalent of half the minimum effective dose of 18-MC. Similarly to 18-MC itself, ME-18-MC acts primarily as a selective αβ nicotinic acetylcholine antagonist, although it has a slightly stronger effect than 18-MC as an NMDA antagonist, and its effects on opioid receptors are weaker than those of 18-MC at all except the kappa opioid receptor, at which it has slightly higher affinity than 18-MC.
I find three 2nd generation congeners: 18-MC, 18-MAC and ME-18-MC. Is that all of these?
Are you set up to develop an analog that people can use safely at home? If so, I'd like to help.
Last edited:
mr peabody
Bluelight Crew
- Joined
- Aug 31, 2016
- Messages
- 5,714
Some other interesting looking papers I found:
18-Methoxycoronaridine, Synthetic iboga alkaloid congener
The ibogaine research team at Albany Medical College has developed a synthetic iboga alkaloid congener, 18-methoxycoronaridine (18-MC). Animal research shows that 18-MC shares ibogaine's anti-addictive properties, possibly without ibogaine's hallucinogenic effects, possibly not.

1. Anti-HIV-1 activity of the Iboga alkaloid congener 18-methoxycoronaridine. Silva, Cirne-Santos, Frugulhetti, Galvao-Castro, Saraiva, Kuehne, Bou-Habib. Planta Med. 2004 Sep; Abstract
2. Anti-addictive actions of an iboga alkaloid congener: a novel mechanism for a novel treatment. Maisonneuve IM, Glick SD. Pharmacol Biochem Behav. 2003 Jun; Abstract
3. Metabolism of 18-Methoxycoronaridine, an Ibogaine Analog, to 18-Hydroxycoronaridine by Genetically Variable CYP2C19. Zhang, Ramamoorthy, Tyndale, Glick, Maisonneuve IM, Kuehne ME, Sellers EM. Drug Metab Dispos 2002 Jun: Abstract
4. Antagonism of alpha3beta4 nicotinic receptors as a strategy to reduce opioid and stimulant self-administration. Glick SD, Maisonneuve IM, Kitchen BA, Fleck MW. Eur J Pharmacol 2002 Mar: Abstract
5. Drug discrimination studies with ibogaine. Helsley S, Rabin RA, Winter JC. Alkaloids Chem Biol 2001; Abstract
6. 18-MC reduces methamphetamine and nicotine self-administration in rats. Glick SD, Maisonneuve IM, Dickinson HA. Neuroreport 2000 Jun: Abstract
7. Pharmacological comparison of the effect of ibogaine and 18-methoxycoronaridine on isolated smooth muscle from the rat and guinea-pig. Mundey MK, Blaylock NA, Mason R, Glick SD, Maisonneuve IM, Wilson VG. Br J Pharmacol 2000 Apr; Abstract
8. Synthesis of enantiomerically pure (+)- and (-)-18-methoxycoronaridine hydrochloride and their preliminary assessment as anti-addictive agents. King CH, Meckler H, Herr RJ, Trova MP, Glick SD, Maisonneuve IM. Bioorg Med Chem Lett 2000 Mar; Abstract
9. 18-Methoxycoronaridine (18-MC) and ibogaine: comparison of antiaddictive efficacy, toxicity, and mechanisms of action. Glick, Maisonneuve, Szumlinsk. Ann N Y Acad Sci 2000; Abstract
10. Development of novel medications for drug addiction. The legacy of an African shrub. Glick SD, Maisonneuve IM. Ann N Y Acad Sci 2000; Abstract*
11. Acute iboga alkaloid effects on extracellular serotonin (5-HT) levels in nucleus accumbens and striatum in rats. Wei, Maisonneuve, Kuehne, Glick. Brain Res 1998 Aug; Abstract
12. Effects of 18-methoxycoronaridine on acute signs of morphine withdrawal in rats. Rho B, Glick SD. Neuroreport 1998 May; Abstract
13. Attenuation of alcohol consumption by a novel nontoxic ibogaine analogue (18-methoxycoronaridine) in alcohol-preferring rats. Rezvani AH, Overstreet DH, Yang Y, Maisonneuve IM, Bandarage UK, Kuehne ME, Glick SD. Pharmacol Biochem Behav 1997 Oct; Abstract
14. Time-dependent interactions between iboga agents and cocaine. Maisonneuve IM, Visker KE, Mann GL, Bandarage UK, Kuehne ME, Glick SD. Eur J Pharmacol 1997 Oct; Abstract
15. 18-Methoxycoronaridine, a non-toxic iboga alkaloid congener: effects on morphine and cocaine self-administration and on mesolimbic dopamine release in rats. Glick SD, Kuehne ME, Maisonneuve IM, Bandarage UK, Molinari HH. Brain Res 1996 May; Abstract
https://ibogainedossier.com/18-mc/index.html
18-Methoxycoronaridine, Synthetic iboga alkaloid congener
The ibogaine research team at Albany Medical College has developed a synthetic iboga alkaloid congener, 18-methoxycoronaridine (18-MC). Animal research shows that 18-MC shares ibogaine's anti-addictive properties, possibly without ibogaine's hallucinogenic effects, possibly not.
1. Anti-HIV-1 activity of the Iboga alkaloid congener 18-methoxycoronaridine. Silva, Cirne-Santos, Frugulhetti, Galvao-Castro, Saraiva, Kuehne, Bou-Habib. Planta Med. 2004 Sep; Abstract
2. Anti-addictive actions of an iboga alkaloid congener: a novel mechanism for a novel treatment. Maisonneuve IM, Glick SD. Pharmacol Biochem Behav. 2003 Jun; Abstract
3. Metabolism of 18-Methoxycoronaridine, an Ibogaine Analog, to 18-Hydroxycoronaridine by Genetically Variable CYP2C19. Zhang, Ramamoorthy, Tyndale, Glick, Maisonneuve IM, Kuehne ME, Sellers EM. Drug Metab Dispos 2002 Jun: Abstract
4. Antagonism of alpha3beta4 nicotinic receptors as a strategy to reduce opioid and stimulant self-administration. Glick SD, Maisonneuve IM, Kitchen BA, Fleck MW. Eur J Pharmacol 2002 Mar: Abstract
5. Drug discrimination studies with ibogaine. Helsley S, Rabin RA, Winter JC. Alkaloids Chem Biol 2001; Abstract
6. 18-MC reduces methamphetamine and nicotine self-administration in rats. Glick SD, Maisonneuve IM, Dickinson HA. Neuroreport 2000 Jun: Abstract
7. Pharmacological comparison of the effect of ibogaine and 18-methoxycoronaridine on isolated smooth muscle from the rat and guinea-pig. Mundey MK, Blaylock NA, Mason R, Glick SD, Maisonneuve IM, Wilson VG. Br J Pharmacol 2000 Apr; Abstract
8. Synthesis of enantiomerically pure (+)- and (-)-18-methoxycoronaridine hydrochloride and their preliminary assessment as anti-addictive agents. King CH, Meckler H, Herr RJ, Trova MP, Glick SD, Maisonneuve IM. Bioorg Med Chem Lett 2000 Mar; Abstract
9. 18-Methoxycoronaridine (18-MC) and ibogaine: comparison of antiaddictive efficacy, toxicity, and mechanisms of action. Glick, Maisonneuve, Szumlinsk. Ann N Y Acad Sci 2000; Abstract
10. Development of novel medications for drug addiction. The legacy of an African shrub. Glick SD, Maisonneuve IM. Ann N Y Acad Sci 2000; Abstract*
11. Acute iboga alkaloid effects on extracellular serotonin (5-HT) levels in nucleus accumbens and striatum in rats. Wei, Maisonneuve, Kuehne, Glick. Brain Res 1998 Aug; Abstract
12. Effects of 18-methoxycoronaridine on acute signs of morphine withdrawal in rats. Rho B, Glick SD. Neuroreport 1998 May; Abstract
13. Attenuation of alcohol consumption by a novel nontoxic ibogaine analogue (18-methoxycoronaridine) in alcohol-preferring rats. Rezvani AH, Overstreet DH, Yang Y, Maisonneuve IM, Bandarage UK, Kuehne ME, Glick SD. Pharmacol Biochem Behav 1997 Oct; Abstract
14. Time-dependent interactions between iboga agents and cocaine. Maisonneuve IM, Visker KE, Mann GL, Bandarage UK, Kuehne ME, Glick SD. Eur J Pharmacol 1997 Oct; Abstract
15. 18-Methoxycoronaridine, a non-toxic iboga alkaloid congener: effects on morphine and cocaine self-administration and on mesolimbic dopamine release in rats. Glick SD, Kuehne ME, Maisonneuve IM, Bandarage UK, Molinari HH. Brain Res 1996 May; Abstract
https://ibogainedossier.com/18-mc/index.html
Last edited:
sekio
Bluelight Crew
- Joined
- Sep 14, 2009
- Messages
- 21,994
Is ibogaine really that cardiotoxic? Presumably taken in flood doses it's not something that needs to be repeatedly administered.
Personally speaking I'd be comfortable with a little transient arrythmia if it meant rapid detoxification from chronic opiate use.
Personally speaking I'd be comfortable with a little transient arrythmia if it meant rapid detoxification from chronic opiate use.
Is ibogaine really that cardiotoxic? Presumably taken in flood doses it's not something that needs to be repeatedly administered.
Personally speaking I'd be comfortable with a little transient arrythmia if it meant rapid detoxification from chronic opiate use.
It is all relative.. in terms of TI, it is probably one of the safest psychoactive, I mean at 2-3gram dosage, most psychoactive would probably kill an average 75 kg person. The issues of cardiac arrythmia has more to do with the rationale given for banning the substance in the US and other countries.. How toxic is ibogaine? (too bad ..thousands are dropping dead that could've benefit from this amazing substance.. too bad).
True, people with preexisting heart problems are at risk of arrythmia at flood doses.. but then again, a lots of used pharmaceuticals drugs (for all kind of conditions) including OTC like common cough syrups do induce hERG blockade ..
^ Wonderful. May I have your permission to re-post that here (bottom): http://www.bluelight.org/vb/threads/823455-Ibogaine-and-opiate-opioid-addiction
Please feel free to use as you see fit (I'll add references later..)
Now as for Coronaridine derivatives like 18-MC, 18-MAC..etc, yeah I am aware of some more derivatives developed by Glicks team. As I said, we have yet to see the effect of "flood dose" of some of those and their effect on long term cessation of opiates, alcohol, meth..etc craving.. All the studies were for opioids acute withdrawals suppression. This is actually not really a big issue to treat with opiates detox. I mean to say NMDA and/or non-selective Nicotinic antagonist such as memantine (and better yet Mecamylamine which is my own suggestion!!) would work just fine or better to treat withdrawals. The question is opiates CRAVING/relapse in the short, medium and long term after detoxiing .. Few drugs (actually none that I am aware of) can suppress CRAVING/relapse following DToxiing similar to Iboagine.. so the issue is really whether 18-MCs have such properties.. anyway interesting compounds..
Depending what you mean by "setup", yeah I am working on safe Ibogaine analogs psychedelic with no cardiovascular side-effects (no ERG channels effect I mean with at least 100xless hERG blockade that Ibogaine but while retaining psychoactivity.. The idea is that people can safely use such analogs at home without worrying about cardiovascular side-effects.. But if you live in the US, keep in mind Ibogaine is scheduled there, therefore illegal so you might be breaking the law .. DM me when you have the chance..Are you set up to develop an analog that people can use safely at home? If so, I'd like to help.
Last edited:
mr peabody
Bluelight Crew
- Joined
- Aug 31, 2016
- Messages
- 5,714
^ Very interesting. If you get a chance to list any more derivatives that would be great. I've re-posted yours to http://www.bluelight.org/vb/threads/...ioid-addiction (thanks!) & I will PM you shortly.
Last edited:
emkee_reinvented
Bluelighter
- Joined
- Jan 27, 2009
- Messages
- 4,178
Thanks liking it.
So the statement "insane in the midbrain" could actually be membrane but who cares
stands https://www.youtube.com/watch?v=zAlNrtcPCLwThat makeover done on Glick in the second link
 is mindblowing. Don't get me wrong he looks ok and his style and goals are a-OK.
is mindblowing. Don't get me wrong he looks ok and his style and goals are a-OK.Weltmeister
Bluelighter
- Joined
- Oct 23, 2015
- Messages
- 231
Unless im mistaken this patent hasnt been mentioned yet. It describes molecules with similar structure to ibogaine which supposedly only have its anti addiction effects.
There are lots of Coronaridine or Ibogaine congeners either natural alkaloids or synthetic derivatives: 18-MC and related Voacangine derivative is one of them .. One alkaloid I found particularly interesting tho is Tabernanthine (which is a positional isomer of ibogaine: It is 11-methoxyibogamine instead of 12-methoxy ibogamine ie ibogaine):^.. If you get a chance to list any more derivatives that would be great...
I am not aware of report of cardiovascular side-effects of tabernanthine like the more common Iboagine: it may (MAY) be less cardiotoxic than ibogaine and its main metabolite noribogaine. It has robust effect on cocaine methamphetamine and morphine WD and cravings similar to ibogaine (cf ref 3 above). Considering that the demand for Ibogaine is decimating the Iboga tree in Africa, Tabernathine can be better alternative to Ibogaine since it is found in larger quantity in trunk barks of Tabernanthe Iboga and also other Tabernanthe species like T. Montana..etc Ibogaine is found only in roots bark of Iboga tree so the tree has to be killed to extract the alkaloid which would lead to the extincion of the species pretty soon considering the huge current demand for Ibogaine in the west.. If anybody have the money and means,Tabernanthine can actually be patented (I mean as a method of use for addiction or microdosing for depression, creativity..etc).. anybody reading this and considering patenting make sure to send me my 15% royalties!!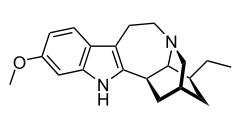
Tabernanthine is an alkaloid found in Tabernanthe iboga.[1]
It has been used in laboratory experiments to study how addiction affects the brain.[2]
Tabernanthine persistently reduced the self-administration of cocaine and morphine in rats.[3]
https://en.wikipedia.org/wiki/Tabernanthine
Last edited:
Unless im mistaken this patent hasnt been mentioned yet. It describes molecules with similar structure to ibogaine which supposedly only have its anti addiction effects.
Thx for pointing out that patent of Ibogaine isoquinuclidine analogs. You are absolutely right: these are ring-opened Ibogaine analogs and could potentially have same effect as Ibogaine. The follow-up study here ( I guess by the same lab)..
Deconstructing the Iboga Alkaloid Skeleton: Potentiation of FGF2-induced Glial Cell Line-Derived Neurotrophic Factor Release by a Novel Compound:
... Glial cell line-derived neurotrophic factor (GDNF), in particular, has been implicated in marked reduction of alcohol consumption in rodent addiction models, and the natural product ibogaine, a substance used traditionally in ritualistic ceremonies, has been suggested to increase the synthesis and release of GDNF in the dopaminergic system in rats. In this report, we describe a novel iboga analog, XL-008, created by unraveling the medium size ring of the ibogamine skeleton, and its ability to induce release of GDNF in C6 glioma cells.... https://pubs.acs.org/doi/10.1021/acschembio.5b00678
Very interesting that single dose of Ibogaine robustly increase neurogenesis in the brain dopaminergic NAC/VTA areas which could explain its long term effect on substance WD/addiction or its anti-Parkinson or other long term benefits.
However, a very recent study claims that Ibogaine metabolite Noribogaine BUT NOT ibogaine is responsible for the robust increase of neurogenesis seen .. here is a summary of the study:
Interesting also to note that psychedelics in general increase neurogenesis and brain plasticity like Ibogaine/noribogaine with LSD having the single most robust increase among psychedelic tested..Psychedelics Promote Structural and Functional Neural Plasticity ( https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6082376/)
Abstract: Atrophy of neurons in the prefrontal cortex (PFC) plays a key role in the pathophysiology of depression and related disorders. The ability to promote both structural and functional plasticity in the PFC has been hypothesized to underlie the fast-acting antidepressant properties of the dissociative anesthetic ketamine. Here, we report that, like ketamine, serotonergic psychedelics are capable of robustly increasing neuritogenesis and/or spinogenesis both in vitro and in vivo. These changes in neuronal structure are accompanied by increased synapse number and function, as measured by fluorescence microscopy and electrophysiology. The structural changes induced by psychedelics appear to result from stimulation of the TrkB, mTOR, and 5-HT2A signaling pathways and could possibly explain the clinical effectiveness of these compounds. Our results underscore the therapeutic potential of psychedelics and, importantly, identify several lead scaffolds for medicinal chemistry efforts focused on developing plasticity-promoting compounds as safe, effective, and fast-acting treatments for depression and related disorders.
Highlights:
Full study here.
- Serotonergic psychedelics increase neuritogenesis, spinogenesis, and synaptogenesis
- Psychedelics promote plasticity via an evolutionarily conserved mechanism
- TrkB, mTOR, and 5-HT2A signaling underlie psychedelic-induced plasticity
- Noribogaine, but not ibogaine, is capable of promoting structural neural plasticity