markosheehan
Bluelighter
- Joined
- Sep 17, 2016
- Messages
- 238
hi
I was reading through these studies on GABAB2 receptors and I am confused.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4205182/
this study is about a girl who had deficient GABAB2 function. This is apparently leading to intellectual problems and seizures. I understand the seizure thing but I always thought a decrease in GABA receptor function leads to increased intellectual capabilities. For example mice with Knockout GABAA 1 and 5 are resistant to cognitive problems brought about by certain Benzos. So is this the other way around/inverse here? or am I just interpreting it wrong here?
this study is about also mutations in GABAB2 function
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5384423/
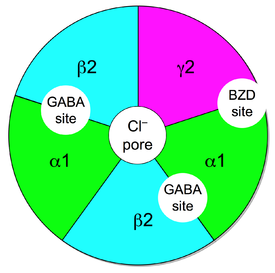
"Here, we report the discovery of a de novo heterozygous missense mutation in the GABRB2 gene that encodes the β2 subunit of the GABAA receptor. Our in vitro studies indicate that this mutation causes EME via disruption of GABAergic inhibition in the brain."
so the people from this case report had seizures due to altered GABAB 2 function like the girl in the first study. But when I relate this back to cognitive problems in the girl it makes no sense to me.
I only have very basic knowledge in this stuff so hopefully your answers can be dumbed down enough for me to understand.
I was reading through these studies on GABAB2 receptors and I am confused.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4205182/
this study is about a girl who had deficient GABAB2 function. This is apparently leading to intellectual problems and seizures. I understand the seizure thing but I always thought a decrease in GABA receptor function leads to increased intellectual capabilities. For example mice with Knockout GABAA 1 and 5 are resistant to cognitive problems brought about by certain Benzos. So is this the other way around/inverse here? or am I just interpreting it wrong here?
this study is about also mutations in GABAB2 function
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5384423/
"Here, we report the discovery of a de novo heterozygous missense mutation in the GABRB2 gene that encodes the β2 subunit of the GABAA receptor. Our in vitro studies indicate that this mutation causes EME via disruption of GABAergic inhibition in the brain."
so the people from this case report had seizures due to altered GABAB 2 function like the girl in the first study. But when I relate this back to cognitive problems in the girl it makes no sense to me.
I only have very basic knowledge in this stuff so hopefully your answers can be dumbed down enough for me to understand.