
- Joined
- Mar 18, 2012
- Messages
- 2,759
Something I found:
Insulin
Too many people fail to understand that that there is much more to the concept of hormones bringing about an effect than simply quantity. Most hormonal effect requires both a hormone and a receptor with which to bind. Most people seem to grasp this much... hormones dock to receptors, locks have no function without keys. This binary model of the world seems to be something easily grasped. Sperm plus egg preceded by vagina plus penis equals procreation... a binary view of the world is built into our DNA and seems to be carried from gene expression yes or no to our everyday decision making.
It takes more than a passing interest for us to understand a topic beyond this yes or no decision matrix. Comprehension takes focus, it takes a bit of effort. It is probably for this reason alone that I have been unwilling to much discuss insulin. Yet insulin should be examined. Not because insulin is unique in the cascade of intracellular events that a binding to it's receptor triggers. Rather It should be examined in part because there are concepts that are common to most hormone-receptor complexes.
In order to understand these common concepts we need to understand that there is more to it then simply the quantity of hormone and the quantity of it's receptor. We need to understand that when a hormone binds to a receptor it does not always result in one outcome. This is such an important concept to understand that I will repeat it. Unlike a key which binds to a lock and produces the singularly consistent outcome of locked or unlocked, hormones often when they bind to their receptor trigger different outcomes. The outcomes are defined in the literature. They are not unknown. Rather they are multiple choice. Whether a hormone ends up triggering outcome A, B or C will depend on several factors some of which are systemic.
However one very easy to understand and perhaps the most significant way a hormone will trigger a specific outcome is the way it binds to a receptor. As an analogy, in a fictional story we may read that a man shakes a woman's hand. From that bare description we visualize a connection made. But was it a brief connection? Was it prolonged? Was it a weak touch or a firm touch? These things are important. How did the hormone bind to the receptor? If it were an insulin handshake with it's receptor did it bring about the uptake of sweet nothings; did it lead to an element of repose where fat liberation was not possible or did it lead to a mitogenic proliferation?
A bit more than binary attention is needed so let's begin.
I will try to keep the science to a minimum. The reason for this is simple. This writing is more about the broader concepts. The broader concepts are in my opinion important in the building of protocols for health & well being as well as for bringing about positive body shape maintenance and change. Betterment in all respects requires that we understand the broader concepts with the understanding that they are built upon detail readily available.
Briefly what does this hormone insulin do in a METABOLIC Way?
Insulin is considered to be the primary hormone controlling "intermediary metabolism". Intermediary metabolism is the intracellular process by which nutritive material is converted into cellular components.
The most noticeable immediate effect on insulin is a lowering of blood glucose.
The primary factor stimulating or failing to stimulate the synthesis and secretion of insulin is the blood glucose concentration.1
Secondary stimuli for insulin release include fatty acids, amino acids (particularly arginine and leucine) and gastrointestinal hormones (such as glucagon-like peptide-1 and gastric inhibitory peptide).
Insulin decreases blood glucose by increasing glucose uptake into muscle and fat cells via GLUT-4 (an insulin-sensitive glucose transporter present in muscle and fat cells), increases glycogen and fatty acids synthesis, DNA replication and protein synthesis, decreases proteolysis, lipolysis, gluconeogenesis and glycogen breakdown. 1
Reference:
1 - Beardsall, K., (2008), Insulin and carbohydrate metabolism, Best Pract. Res. Clin. Endocrinol. Metab. 22, 41?55
Insulin's Mitogenic Way?
If something is mitogenic it acts to encourage cells to begin cell division and enter the process that multiplies cells. The term is often used in regard to the growth of tumors. At times it may be misapplied to muscle acquisition. Muscle acquisition requires the making of proteins which can be incorporated into existing muscle structure. To expand the ability to do that the machinery components (primarily nuclei) are multiplied or proliferated and donated to existing muscle cell structures.
Whether "the mitogenic way" is good or bad depends on where and when it acts. To grow a fetus or repair a wound would be characterized as good. To grow a tumor would be bad. Controlled "mitogenic ways" are necessary to maintain us in healthy ways.
One way this process seems to be controlled is through the Globalge of preferred hormones in the proper tissue to trigger the process of proliferation. If we look inside a cell we can see the signalling pathway that triggers cellular proliferation. The pathway that involves the elements RAS -> ERK 1/2 is a "mitogenic way" that can lead to cellular proliferation. These same elements can be triggered by growth hormone, Insulin-like growth factor I, Insulin-like growth factor II or insulin. However it is best not to trigger these elements in the wrong tissue or at the wrong time.
In specific conditions like cancer and diabetes, the insulin receptor may acquire the ability to stimulate cell proliferation. This acquired ability may be thought of as a functional switch. Attempting to understand how that functional switch is triggered is important because insulin has beneficial roles to play which can be maximized or utilized to one's benefit. Benefit may require avoiding insulin triggered "mitogenic way" .
Metabolic/Mitogenic ratio
When we speak of insulin we refer to native insulin and the exogenously administered analogs. Humulin is the closest to native insulin and for the most part can be thought to have the same metabolic/mitogenic ratio. Using human insulin as a baseline Humalog has been found to exhibit a similar metabolic profile. Glucose transport and lipogenesis for example were found to be equivalent. Humalog has also been found to exhibit the same mitogenic potency in non-malignant and malignant tissue. Inhibition of apoptosis was also similar to human insulin.
The longer lasting, slow acting insulins that raise base insulin levels (glargine (Lantus?), and insulin detemir (Levemir?) seem to have increased mitogenic potency in malignant cells. 2
In my opinion this also underscores what happens when you raise base levels of native insulin. You increase "the mitogenic way"
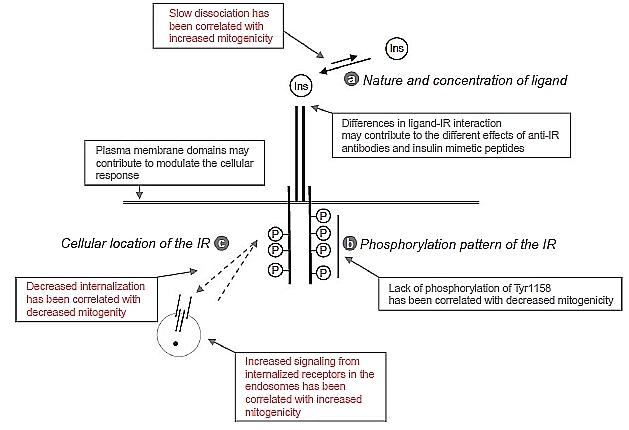
What increases "the mitogenic way"?
It appears that insulin that dissociates very slowly from the receptor creates a sustained activation of the insulin receptor and sustained phosphorylation of Shc. See the mitogenic pathway Basically the longer insulin stays bound to it's receptor the more likely that the fundamental switch will be triggered from metabolic to mitogenic activity. The bound insulin-insulin receptor complex can become internalized into the cell. Some studies show a correlation between the internalization of the insulin analogs and the activation of the mitogenic pathway. High internalization of insulin-insulin receptor rates correlate with higher Shc phosphorylation and ERK activation whereas a low internalization rate correlated with marginal activation of ERK. These are the proliferative pathways. In addition prolonged receptor binding decreases insulin degradation. 3-5
It is important to also note that any increased interaction with the IGF1 receptor may also contribute to the higher mitogenicity.6
References:
2 - Differences in bioactivity between human insulin and insulin analogues approved for therapeutic use compilation of reports from the past 20 years, Haim Werner, Diabetology & Metabolic Syndrome 2011, 3:13
3 - The bioactivity of insulin analogues from in vitro receptor binding to in vivo glucose uptake, Drejer, K., Diabetes Metab. Rev. 8, 259?285 1992
4 - Insulin and IGF-1 receptor trafficking and signalling, Foti, M., Novartis Found. Symp. 262, 125?141 (2004)
5 - A novel insulin analog with unique properties: LysB3,GluB29 insulin induces prominent activation of insulin receptor substrate 2, but marginal phosphorylation of insulin receptor substrate 1, Rakatzi, I., Diabetes 52, 2227?2238 (2003)
6 - Correlations of receptor binding and metabolic and mitogenic potencies of insulin analogs designed for clinical use, Kurtzhals, P., Diabetes 49, 999?991005 (2002)
To reiterate the actions of Insulin
When you are putting together a protocol that involves insulin, whether it be inducing native insulin release or using exogenous insulin, you need to keep in mind precisely what it is that you are attempting to accomplish during that moment. Are you attempting to induce anti-apoptosis, increase glycogen uptake, effect protein synthesis? Are you trying to effect gene expression? If so which? for instance are you attempting to prepare the body to respond more vigorously to the next round of growth hormone pulse? If so are you attempting to refresh a Stat5b response? Are you attempting to increase GH receptors in anticipation of an artificially induced GH pulse?
Are you trying to increase the release of fatty acids? If so insulin gets in the way.
Finally are you attempting to engage a mitogenic response? If so understand that much of the time insulin as a standalone way to activate the proliferative machinery is a potentially unhealthy approach. Far better to either avoid triggering that pathway with insulin or only use it sparingly as support for activation of those proliferative pathways via other hormone-receptor complexes.
Most importantly we do have an element of control over how this hormone (as well as others) will behave. By choosing the when, by choosing the type (i.e. pulses or elevations), by choosing the analogs and by fitting the hormone into an overall protocol where the hormone is expected to contribute to only a part of the overall strategy we can exert some sort of control over how the hormone will behave.
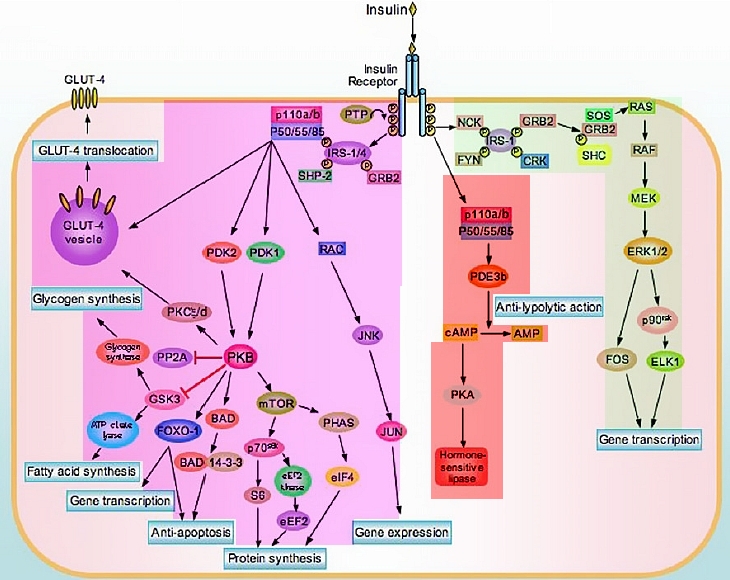
Schematic representation of IR signalling. Insulin binding leads to receptor autophosphorylation and phosphorylation of several intracellular substrates including IRS1/4. Phosphorylated IRS-1 recruits Grb2/Sos complex, which triggers the RAS/RAF/MEK/ERK pathway (on the right). This pathway is mainly involved in mediating the mitogenic effect of insulin and insulin like growth factors (IGF-I and IGF-II). Recruitment of p85 on IRS-1 and IRS-2 leads to PI-3 kinase activation, and, as a consequence, Akt pathway activation and Glut4 translocation (on the left). This pathway is mainly involved in mediating the metabolic effects of insulin, including glucose uptake, glycogen and protein synthesis. Moreover, Akt pathway activation is responsible for the anti-apoptotic effect of insulin, IGF-I and IGF-II.
Insulin
Too many people fail to understand that that there is much more to the concept of hormones bringing about an effect than simply quantity. Most hormonal effect requires both a hormone and a receptor with which to bind. Most people seem to grasp this much... hormones dock to receptors, locks have no function without keys. This binary model of the world seems to be something easily grasped. Sperm plus egg preceded by vagina plus penis equals procreation... a binary view of the world is built into our DNA and seems to be carried from gene expression yes or no to our everyday decision making.
It takes more than a passing interest for us to understand a topic beyond this yes or no decision matrix. Comprehension takes focus, it takes a bit of effort. It is probably for this reason alone that I have been unwilling to much discuss insulin. Yet insulin should be examined. Not because insulin is unique in the cascade of intracellular events that a binding to it's receptor triggers. Rather It should be examined in part because there are concepts that are common to most hormone-receptor complexes.
In order to understand these common concepts we need to understand that there is more to it then simply the quantity of hormone and the quantity of it's receptor. We need to understand that when a hormone binds to a receptor it does not always result in one outcome. This is such an important concept to understand that I will repeat it. Unlike a key which binds to a lock and produces the singularly consistent outcome of locked or unlocked, hormones often when they bind to their receptor trigger different outcomes. The outcomes are defined in the literature. They are not unknown. Rather they are multiple choice. Whether a hormone ends up triggering outcome A, B or C will depend on several factors some of which are systemic.
However one very easy to understand and perhaps the most significant way a hormone will trigger a specific outcome is the way it binds to a receptor. As an analogy, in a fictional story we may read that a man shakes a woman's hand. From that bare description we visualize a connection made. But was it a brief connection? Was it prolonged? Was it a weak touch or a firm touch? These things are important. How did the hormone bind to the receptor? If it were an insulin handshake with it's receptor did it bring about the uptake of sweet nothings; did it lead to an element of repose where fat liberation was not possible or did it lead to a mitogenic proliferation?
A bit more than binary attention is needed so let's begin.
I will try to keep the science to a minimum. The reason for this is simple. This writing is more about the broader concepts. The broader concepts are in my opinion important in the building of protocols for health & well being as well as for bringing about positive body shape maintenance and change. Betterment in all respects requires that we understand the broader concepts with the understanding that they are built upon detail readily available.
Briefly what does this hormone insulin do in a METABOLIC Way?
Insulin is considered to be the primary hormone controlling "intermediary metabolism". Intermediary metabolism is the intracellular process by which nutritive material is converted into cellular components.
The most noticeable immediate effect on insulin is a lowering of blood glucose.
The primary factor stimulating or failing to stimulate the synthesis and secretion of insulin is the blood glucose concentration.1
Secondary stimuli for insulin release include fatty acids, amino acids (particularly arginine and leucine) and gastrointestinal hormones (such as glucagon-like peptide-1 and gastric inhibitory peptide).
Insulin decreases blood glucose by increasing glucose uptake into muscle and fat cells via GLUT-4 (an insulin-sensitive glucose transporter present in muscle and fat cells), increases glycogen and fatty acids synthesis, DNA replication and protein synthesis, decreases proteolysis, lipolysis, gluconeogenesis and glycogen breakdown. 1
Reference:
1 - Beardsall, K., (2008), Insulin and carbohydrate metabolism, Best Pract. Res. Clin. Endocrinol. Metab. 22, 41?55
Insulin's Mitogenic Way?
If something is mitogenic it acts to encourage cells to begin cell division and enter the process that multiplies cells. The term is often used in regard to the growth of tumors. At times it may be misapplied to muscle acquisition. Muscle acquisition requires the making of proteins which can be incorporated into existing muscle structure. To expand the ability to do that the machinery components (primarily nuclei) are multiplied or proliferated and donated to existing muscle cell structures.
Whether "the mitogenic way" is good or bad depends on where and when it acts. To grow a fetus or repair a wound would be characterized as good. To grow a tumor would be bad. Controlled "mitogenic ways" are necessary to maintain us in healthy ways.
One way this process seems to be controlled is through the Globalge of preferred hormones in the proper tissue to trigger the process of proliferation. If we look inside a cell we can see the signalling pathway that triggers cellular proliferation. The pathway that involves the elements RAS -> ERK 1/2 is a "mitogenic way" that can lead to cellular proliferation. These same elements can be triggered by growth hormone, Insulin-like growth factor I, Insulin-like growth factor II or insulin. However it is best not to trigger these elements in the wrong tissue or at the wrong time.
In specific conditions like cancer and diabetes, the insulin receptor may acquire the ability to stimulate cell proliferation. This acquired ability may be thought of as a functional switch. Attempting to understand how that functional switch is triggered is important because insulin has beneficial roles to play which can be maximized or utilized to one's benefit. Benefit may require avoiding insulin triggered "mitogenic way" .
Metabolic/Mitogenic ratio
When we speak of insulin we refer to native insulin and the exogenously administered analogs. Humulin is the closest to native insulin and for the most part can be thought to have the same metabolic/mitogenic ratio. Using human insulin as a baseline Humalog has been found to exhibit a similar metabolic profile. Glucose transport and lipogenesis for example were found to be equivalent. Humalog has also been found to exhibit the same mitogenic potency in non-malignant and malignant tissue. Inhibition of apoptosis was also similar to human insulin.
The longer lasting, slow acting insulins that raise base insulin levels (glargine (Lantus?), and insulin detemir (Levemir?) seem to have increased mitogenic potency in malignant cells. 2
In my opinion this also underscores what happens when you raise base levels of native insulin. You increase "the mitogenic way"
What increases "the mitogenic way"?
It appears that insulin that dissociates very slowly from the receptor creates a sustained activation of the insulin receptor and sustained phosphorylation of Shc. See the mitogenic pathway Basically the longer insulin stays bound to it's receptor the more likely that the fundamental switch will be triggered from metabolic to mitogenic activity. The bound insulin-insulin receptor complex can become internalized into the cell. Some studies show a correlation between the internalization of the insulin analogs and the activation of the mitogenic pathway. High internalization of insulin-insulin receptor rates correlate with higher Shc phosphorylation and ERK activation whereas a low internalization rate correlated with marginal activation of ERK. These are the proliferative pathways. In addition prolonged receptor binding decreases insulin degradation. 3-5
It is important to also note that any increased interaction with the IGF1 receptor may also contribute to the higher mitogenicity.6
References:
2 - Differences in bioactivity between human insulin and insulin analogues approved for therapeutic use compilation of reports from the past 20 years, Haim Werner, Diabetology & Metabolic Syndrome 2011, 3:13
3 - The bioactivity of insulin analogues from in vitro receptor binding to in vivo glucose uptake, Drejer, K., Diabetes Metab. Rev. 8, 259?285 1992
4 - Insulin and IGF-1 receptor trafficking and signalling, Foti, M., Novartis Found. Symp. 262, 125?141 (2004)
5 - A novel insulin analog with unique properties: LysB3,GluB29 insulin induces prominent activation of insulin receptor substrate 2, but marginal phosphorylation of insulin receptor substrate 1, Rakatzi, I., Diabetes 52, 2227?2238 (2003)
6 - Correlations of receptor binding and metabolic and mitogenic potencies of insulin analogs designed for clinical use, Kurtzhals, P., Diabetes 49, 999?991005 (2002)
To reiterate the actions of Insulin
When you are putting together a protocol that involves insulin, whether it be inducing native insulin release or using exogenous insulin, you need to keep in mind precisely what it is that you are attempting to accomplish during that moment. Are you attempting to induce anti-apoptosis, increase glycogen uptake, effect protein synthesis? Are you trying to effect gene expression? If so which? for instance are you attempting to prepare the body to respond more vigorously to the next round of growth hormone pulse? If so are you attempting to refresh a Stat5b response? Are you attempting to increase GH receptors in anticipation of an artificially induced GH pulse?
Are you trying to increase the release of fatty acids? If so insulin gets in the way.
Finally are you attempting to engage a mitogenic response? If so understand that much of the time insulin as a standalone way to activate the proliferative machinery is a potentially unhealthy approach. Far better to either avoid triggering that pathway with insulin or only use it sparingly as support for activation of those proliferative pathways via other hormone-receptor complexes.
Most importantly we do have an element of control over how this hormone (as well as others) will behave. By choosing the when, by choosing the type (i.e. pulses or elevations), by choosing the analogs and by fitting the hormone into an overall protocol where the hormone is expected to contribute to only a part of the overall strategy we can exert some sort of control over how the hormone will behave.
Schematic representation of IR signalling. Insulin binding leads to receptor autophosphorylation and phosphorylation of several intracellular substrates including IRS1/4. Phosphorylated IRS-1 recruits Grb2/Sos complex, which triggers the RAS/RAF/MEK/ERK pathway (on the right). This pathway is mainly involved in mediating the mitogenic effect of insulin and insulin like growth factors (IGF-I and IGF-II). Recruitment of p85 on IRS-1 and IRS-2 leads to PI-3 kinase activation, and, as a consequence, Akt pathway activation and Glut4 translocation (on the left). This pathway is mainly involved in mediating the metabolic effects of insulin, including glucose uptake, glycogen and protein synthesis. Moreover, Akt pathway activation is responsible for the anti-apoptotic effect of insulin, IGF-I and IGF-II.