Where in addiction science is the loss of self-control?
A brief history of biomedical approaches to addiction
A few early modern authorities dabbled with the idea that inebriety may be a disease (cf. Levine, 1978; Porter, 1985), but sustained biomedical interest did not emerge until the middle of the nineteenth century. By the late nineteenth century there was a fairly well established two tiered medical understanding of addic- tion (Courtwright, 2001). Those who could afford private care were ordinarily diagnosed with the so-called disease of neurasthenia, lit- erally nervous exhaustion, and prescribed temporary respite from the complex demands of modern life. Those who could not afford to pay were consigned to state sponsored institutions also staffed by medical doctors but designed to manage the more pessimistic diag- nosis of degeneracy. Degeneracy followed either from a hereditary predisposition or a dissolute life and while it could be prevented, few medical men thought it could be reversed. Rather than seeking to return the patient to a former state of non-addiction, the medical treatment of degeneracy was focused more on limiting the havoc degenerate addicts might wreak upon their wider communities.
In these early days, reigning theories still reflected the influ- ences of humoral medicine in prioritising attention to moderate habits and self-regulation over anatomical structure and physio- logical function. And while it would be unfair to blithely reduce nineteenth century addiction medicine to no more than dressed- up social prejudices, it was undeniably more deeply informed by the perceived character of the patient than the perceived character of his or her putative disease (Baumohl & Room, 1987; Courtwright, 2001). In short, insofar as addiction medicine had not yet fully dis- tinguished medical pathology from the social marginality it was meant to explain, it had as yet no clear separation between what a Foucauldian might call the biomedical and the socio-cultural gaze. Nor, more specifically, did it provide any way of medically linking drug use with a loss of self-control. Neurasthenia cast addiction as a form of fatigue not biological dysfunction and, likewise, degeneracy yielded an understanding of addiction as atavism not affliction. Nei- ther could empirically distinguish self-control from its loss because in neither case was anything other than the self of the supposed addict implicated as a proximal cause of his or her behaviour.
As the nineteenth century came to a close, addiction medicine entered a protracted period of doldrums. Theories of degeneracy and neurasthenia were eventually dismissed by a new genera- tion of medical scientists and the pall of prohibitionist sentiment and then legislation both minimised the availability of funding for addiction research and dissuaded most medical professionals from entering the field. Those who did occupied two camps. The first embraced psychodynamic theories that retained a view of addicts as intrinsically inferior beings (cf. Acker, 2002). The sec- ond focused on physiological withdrawal, arguing that addiction did not belie underlying deficits like degeneracy or psychopathy but was a normal physiological response to which anyone might succumb (Campbell, 2007). Because they seemed to legitimate medical maintenance of addicts’ drug supply, physiological with- drawal based theories did not enjoy much approval amongst policy makers committed to prohibition but did slowly gain sway in the medical community as psychodynamic psychiatry fell from favour. Physiological withdrawal symptoms appeared to provide a specific, universally applicable, biomedically identifiable marker by which addicts might be categorically distinguished from non-addicts. They thereby introduced an apparent path to scientific respectabil- ity insofar as the aetiology and identity of addiction could now be categorically specified in strictly biomedical terms. Those sub- stances that produce physiological withdrawal symptoms were classed as genuinely addictive. Those that did not were categori- cally denied that status. However, once again, addiction science had plainly failed to link drug use with a loss of self-control. Demon- strating that a substance causes withdrawal symptoms does not indicate how these symptoms, in turn, cause a loss of self-control rather than just a change and narrowing of personal priorities.1 Indeed, using drugs to stave off the pains of withdrawal could be seen to exhibit a perfectly reasonable cost–benefit analysis.
Other, better noticed, anomalies began to accumulate too. One can perfectly understand how someone might remain in a per- petual cycle of withdrawal symptom avoidance for as long as withdrawal symptoms actually loom. But why is it, some asked, that the many medications that ease or altogether eliminate physiologi- cal withdrawal symptoms have had such a dismal record of getting people permanently off drugs? Perhaps even more perplexing, why are those who have actually suffered the ravages of cold turkey not uniformly chastened by this experience? One would think that such a profoundly nasty ordeal might discourage people from returning to the use of physically addictive drugs. But, too often, it does no such thing. Conversely, why do so many people who become phys- iologically dependent seem to have so few, if any, qualms about stopping? Finally, it has grown progressively more difficult to argue that only gross physiological withdrawal symptoms2 cause addic- tion. Drugs like crack cocaine or nicotine and activities like sex, gambling, and eating – none of which produce such symptoms – appear capable of inducing behavioural patterns every bit as dam- aging as those induced by alcohol and opiates. It is in no small part due to this accumulation of anomalies that interest turned to our most recent paradigm in biomedical addiction science (cf. Leshner, 1997, p. 46), what the historian David Courtwright (2010) dubbed the “NIDA Brain Disease Paradigm.”
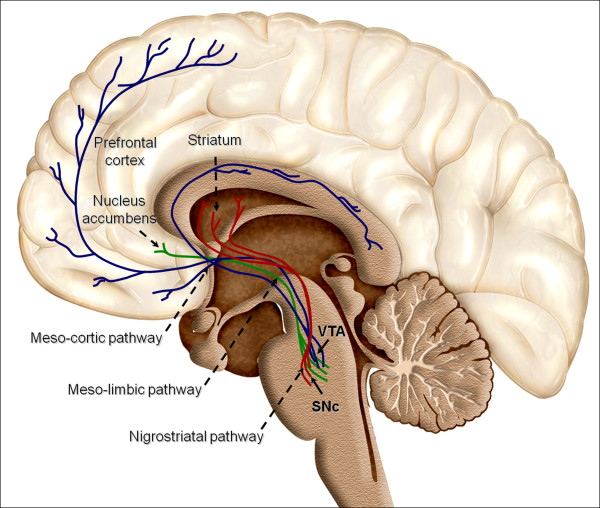
The brain disease paradigm is first and foremost anchored in the priority given to basic science (Campbell, 2010; Vrecko, 2010). This has largely meant confining research to basic biology conceived as a primordial, discrete and independently integrated ontological domain. Brain disease scientists argue that people ingest chemicals like heroin, cocaine, alcohol or nicotine because they biologically cause euphoria by promoting the release of neurotransmitters, pre- venting their re-uptake, or mimicking their effects (cf. Koob, 2006). But what of addiction? Many studies have noted after prolonged use the positive effects of drug use are often eclipsed by the negative (cf. Koob, Stinus, LeMoal, & Bloom, 1989). Some heavy users even report that they continue to relapse despite the fact that drugs have long since ceased to give them any satisfaction at all (cf. Lindesmith, 1968). How does the brain disease paradigm account for these seemingly anomalous findings? It does so by suggesting prolonged drug use induces neurological adaptations that both reduce users’ sensitivity to alternative sources of reward and increase sensitivity to the anticipated rewards of drug use. While these adaptations do not produce gross withdrawal symptoms upon cessation of use, they do render people considerably more vulnerable than they might otherwise be to relapse.
How does this model account for addicts’ putative loss of self-control? First, according to incentive sensitization theory, the intensity of addicts’ desire for drugs is neurologically disjoined from the degree to which they derive pleasure from drug use (cf. Robinson & Berridge, 2003). Hence, their felt desire for drugs is apparently unjustified by the degree of benefit users believe they derive from them. This finding has prompted brain disease scien- tists to cast this desire as pathological by virtue of its inconsistency with conventional understandings of rational choice. But conflating the perception of self-control with an abstract model of rational choice is scientifically unsustainable. Discounting future outcomes in favour of expectations of short term satisfactions does not logically entail a loss of self-control nor do people necessarily experience it as such. People often throw caution to the wind with no ensuing inference that they have been pathologically deprived of their self-control. Aside from denigrating their judgement, an adequate scientific account of the loss of self-control must explain why and how peo- ple appear to grow estranged from their own behaviour enough to warrant the claim that they are genuinely afflicted by some- thing rather than merely exercising limited foresight (Weinberg, 2005).
The second way neurological adaptations to drug use are said to deprive people of their self-control is by compromising brain pro- cesses associated with what are often called executive functions (cf. Goldstein & Volkow, 2011).3 These functions are not always clearly delineated in the brain disease literature, but they cover things like attention, response inhibition, planning, problem solving, working memory, and other such meta-cognitive matters pertaining to the evaluation and control of first order cognitive processes. Like incen- tive sensitization theory, this research seeks universal neurological measures of self-control. While they may have other scientific mer- its, such efforts invariably stray rather far from the lived realities and experiences of self-control and its loss amongst humans out- side lab settings. To claim that people uniformly equate their own or each other’s self-control with their capacities for long term planning, problem solving and impulse control would be patently false. Not only do we deliberately throw caution to the wind on occasion but so too on occasion do we equate our “real selves” with our gut instincts, spontaneous sensibilities or predilections and indeed equate the kinds of activities associated with “executive function” with alien- ation from our real selves and authentic self-control (cf. Alasuutari, 1992, pp. 160–161; Hochschild, 2012; Turner, 1976). Indeed pre- cisely because they hope to re-establish people’s authentic sense of themselves, many rehabilitation programmes place extensive therapeutic emphasis not on learning to executively inhibit sponta- neous emotions but on “getting in touch” with them through their free and open expression.
This neuroscientific disregard for the manifold empirical permu- tations of self-control and the loss thereof stems from a manifest inability or unwillingness to breach the boundaries of brain biol- ogy in any but the most ancillary manner. The brain disease of addiction is held to occur wholly within the confines of an evo- lutionarily determined organismic system that all members of our species share more or less in common. Yes, this system interacts with the environment in which it must survive but it does so in a manner pre-programmed by the legacy of its evolution and largely fixed by genetic inheritance. While conditioning may arbitrarily link environmental cues with our experience of substances and/or activities deemed intrinsically addictive, it poses no prospect of fundamental divergences between the neurological characteristics of either sufferers or their brain diseases themselves. Instead, con- ditioning yields only secondary elaborations precisely analogous to the more general relationship neuroscientists draw between the singularity and determinacy of our biological nature as a species and the diversity and impermanence of the cultures we inhabit. In any event, both brain function and dysfunction are understood as mechanically caused by a combination of biological and ecologi- cal determinants and, hence, seemingly, nondiscretionary whether addicted or not. This mindset will no doubt continue to yield scien- tific dividends in a variety of ways. But because it does not speak to the physiology underlying the diverse empirical permutations of freedom or self-control in the first place, it cannot yield a scientifi- cally valid grasp of the nuanced phenomenology of being estranged from one’s own behaviour – that is, losing self-control – nor the jointly intrapersonal, interpersonal and social structural dynamics that render that estrangement so real for people.