llamer
Bluelighter
I can't tell if the sedative properties of certain antihistamines results from their H1 antagonism or if it's because of their cross effect with antagonizing the adrenergic receptors. Are all H1 antagonists innately sedating or is it just the first generation ones? Anyway I'd like to know which of them (regardless as their branding as 'antihistamines') has the strongest affiliations with these receptors known for producing hypnotic properties.
From what I can tell I think the list beginning with the strongest goes something like this:
Quetiapine (seroquel)
Mirtazipine (remeron)
(from experience)
Hydrazine
Promethazine
(from inference from the internet's experience)
---------
Anything else I'm missing here?
---------
IMHO dipenhydramine, trazadone and haldol are not even worthy of placing on this list, unless you like restless leg syndrome and feeling like a mental ward patient. Even seroquel at tolerance-level dosing gave me very uncomfortable nightmarish RLS/insomnial hellacious torture that I would never wish to endure ever again. My only interest here is to know what works acutely and is not going to pussyfoot around. I've taken both remeron and seroquel but I can't for the life of me determine which of them is technically the stronger sedative (aside from relative dose) because the time between taking them has been too long to compare.
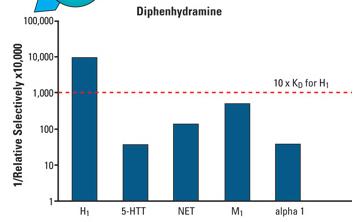
Just wondering if someone could supply some binding affinity charts to this thread. Thanks.
From what I can tell I think the list beginning with the strongest goes something like this:
Quetiapine (seroquel)
Mirtazipine (remeron)
(from experience)
Hydrazine
Promethazine
(from inference from the internet's experience)
---------
Anything else I'm missing here?
---------
IMHO dipenhydramine, trazadone and haldol are not even worthy of placing on this list, unless you like restless leg syndrome and feeling like a mental ward patient. Even seroquel at tolerance-level dosing gave me very uncomfortable nightmarish RLS/insomnial hellacious torture that I would never wish to endure ever again. My only interest here is to know what works acutely and is not going to pussyfoot around. I've taken both remeron and seroquel but I can't for the life of me determine which of them is technically the stronger sedative (aside from relative dose) because the time between taking them has been too long to compare.
Just wondering if someone could supply some binding affinity charts to this thread. Thanks.