Is it perhaps then that the effects of SSRI's are seen predominately in an area of the brain which is not strongly associated with motivation? Is there some other confounding factor i have overlooked?
but tbph you'll find reductive theories throughout psychopharmacology - there isn't a lot of hard science out there on it.
Believe me when i say i know this to be true. Honestly though it shouldn't be too much longer before we just unravel a brain entirely and determine the purpose of various interrelations mathematically. We've had the electron microscope for nearly a century now and with the LHC continuing to produce data i can't imagine a neutrino microscope is far off which should finally allow us to observe (approximately) the atomic level since it would pretty much catch-22 out of heisenberg's famous uncertainty principle.
We really do live in an exciting time, the the proverbial blank edges of the map are filling in and the age of psychological speculation is fast drawing to a close.
Imagine what will be possible in a world where a theory of everything has fully united all of science and we have the human brain mapped to the last picometer.
Imagine a theory of emotion in terms of Maxwell's three laws of thermodynamics!
Imagine that serendipitous drug discovery will fall as a relic of the past to systemic drug synthesis founded in an intimate knowledge of
every protein's shape, function and composition. Compounds mathematically calibrated for effects so precise that they could be individually tailored to a single person's needs. Mental illnesses that are physical rather then psychosomatic would cease to exist, and even psychosomatic ones could be mitigated beyond notice with therapy so profoundly understanding as to transcend description.
We could solve the local problem (read: every problem that actually concerns us in terms of there's not enough energy to go around) within the next three generations; suffering of all kinds could be banished from the lives of those who so wish. Unlimited life-spans, unlimited energy, unlimited progress; constrained only by the pauli-exclusion principle (things take up space) and causality (Something can Cause something else) we could have anything and everything and a near eternity to solve the global problem. (Read: Usable energy is a finite, decreasing number, while the expansion of space is accelerating and removing objects from causal connection with each other, or more simply the ultimate eventuality of the universe seems to be a universe made only of useless energy in regions that physically can not interact. So whether we starve or tear apart at the sub-atomic level first, the global problem is really gonna suck at least 10^100 years from now.) Beyond that there is only apotheosis, perfection, infinity, the shedding of our mortal coils and depending on who you ask there's lotsa trumpets, fields of reeds, Alphas, omegas, epsilon's, clouds, fires, Everything, nothing, cherry-pie, angels, totality, no cherry-pie, peace, tranquility, and god-willing no transcendental-divine problem in which were' running out of real numbers to use or multiplication breaks or something. Then again maybe the problems are kinda fun and self-actualizing? I guess we'll cross that bridge when we get to it! Ordem e Progresso my friends. /end speed rant /Gratitude for indulging me
")

TL: DR
Tomorrows science is today's fiction and yesterday's magic. Also i latently brag about knowing physics terms to a predominately chem/bio audience, make subtle self-avowedly clever jokes of an incredibly technical nature, want a mass-energy conversion engine really bad, reference an obscure national motto digress, regress, progress, digress again, egress, express, profess, obsess, impress, and finally confess that this last bit wasn't clever at all and that i've wholly misunderstood the purpose of a TL: DR.
TL: DR for TL: DR
I'm bored, speeding and think I'm way more interesting and clever then i am.
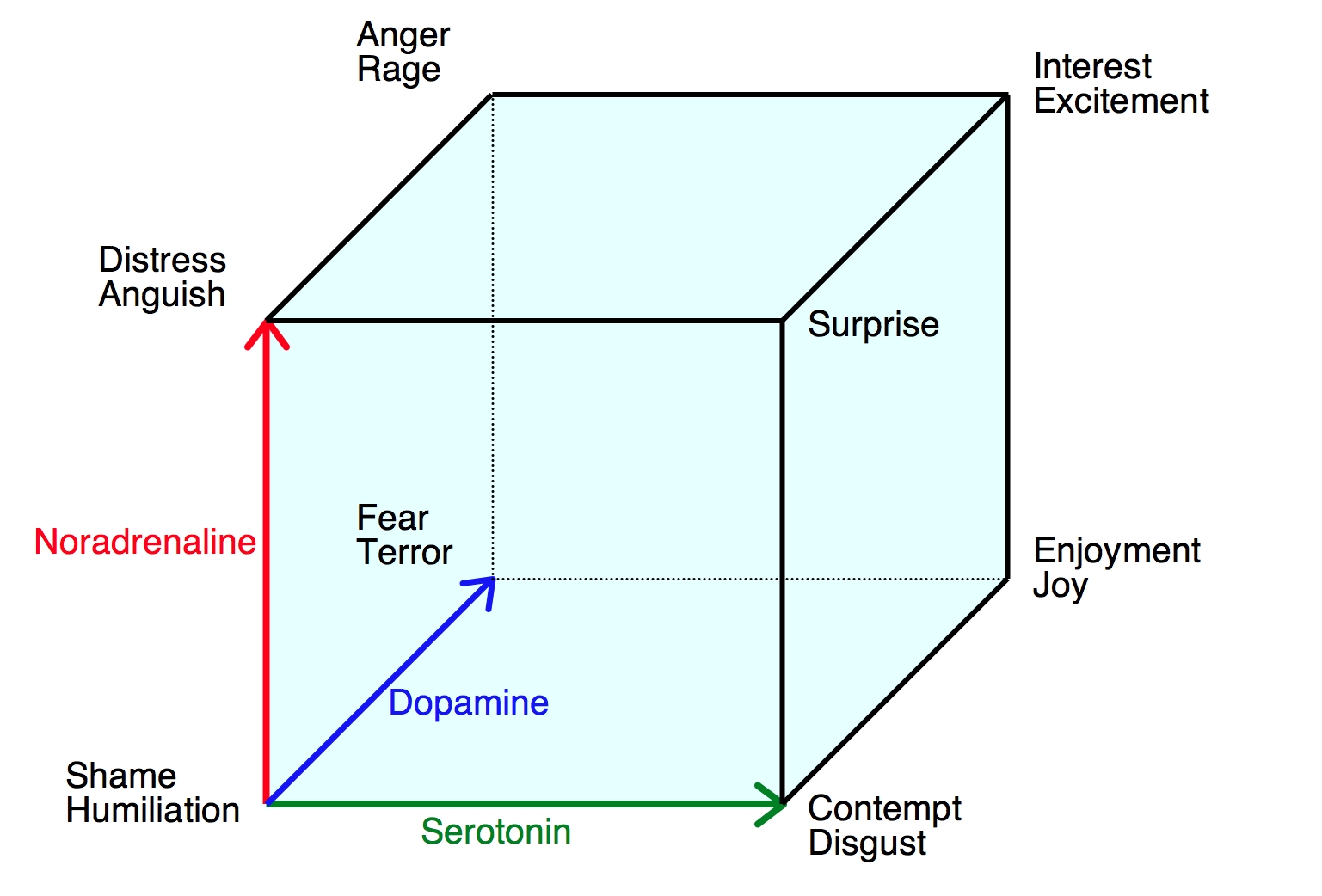
I do so love cubes. They very rarely fail to delight.
You wouldn't risk "serotonin poisoning" unless you're taking a loooot of amphetamine or meth
1) Observe above speed rant as well as unnecessarily complex and pedantic diction and syntax throughout writing. 2) Consider also the prospective motivation for construing a post of this topic and the number of pointless digressions. 3) Draw own conclusions; or maybe even paint them if you're feeling creative.
Disclaimer
*Xeromatosis LLC does not endorse, recommend, or encourage excessive use of addictive and potentially harmful substances and discourages anyone from breaking local laws or chasing local, magical dragons. Always follow your doctor's instructions when taking medication.*
Its probably best suited for OD. I don't think ADD is a bad place for it but they tend to not answer questions over there which 95% of the drug-taking population finds useful. Some of them are elitist pigs too (Hammilton, pretty much (luckily he's not on often)).
The best way to deal with elitists is to let them think whatever they want about their relative self-worth, It's no skin of my back if someone derives self-confidence through arbitrarily demeaning users of an internet forum. Maybe i even made their day a little bit better by allowing them to profess their contempt for me!
Retrospectively this post is largely conversational and off-topic yet amuses me far too much to edit down, so i reiterate:
Is it perhaps then that the effects of SSRI's are seen predominately in an area of the brain which is not strongly associated with motivation? Is there some other confounding factor i have overlooked? Do the mechanisms of the two drugs actions fall in some way counterpoint to each other such as to not combine additively or multiplicatively? A brief explanation of the fatal flaw in this concept's logic or link to literature explaining the same would be greatly appreciated. Bonus points for relevant cube graphics and/or impressive looking hard data. %)