

thegreenhand
Bluelight Crew
So we've all seen numbers like the ones in this table:
 ibb.co
ibb.co
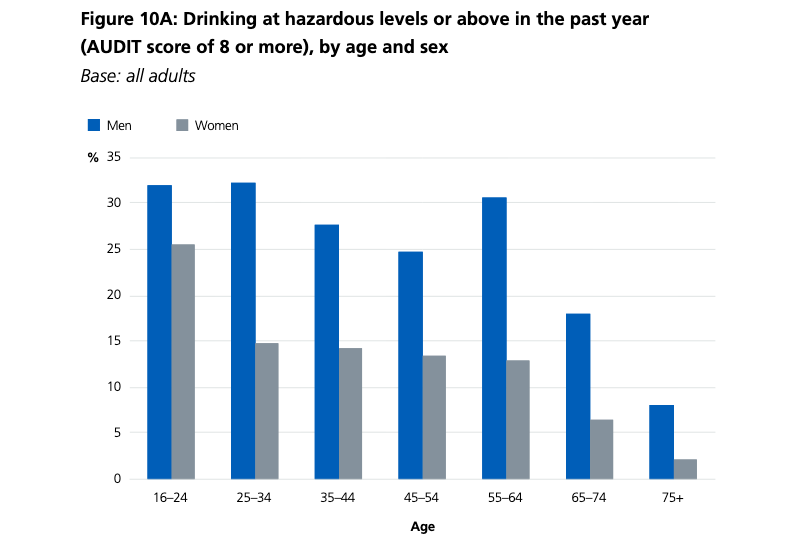
source: https://files.digital.nhs.uk/pdf/r/1/adult_psychiatric_study_ch10_web.pdf
Percentages of adults who have use a given drug, and then also go on to abuse it. What I'm wondering, is how useful are these measures for determining the "abuse potential" of a drug? Finding a table of drugs vs. their abuse potential has proven very difficult, and I'm wondering why this is. Lack of funding or lack of usefulness?
Screen-Shot-2020-12-10-at-7-09-29-PM hosted at ImgBB
Image Screen-Shot-2020-12-10-at-7-09-29-PM hosted in ImgBB
ibb.co
source: https://files.digital.nhs.uk/pdf/r/1/adult_psychiatric_study_ch10_web.pdf
Percentages of adults who have use a given drug, and then also go on to abuse it. What I'm wondering, is how useful are these measures for determining the "abuse potential" of a drug? Finding a table of drugs vs. their abuse potential has proven very difficult, and I'm wondering why this is. Lack of funding or lack of usefulness?
