Metabotropic Glutamate Receptors type 5 (mGluR5)-null mice do not show any reinforcing effects with neither opioids (heroine) or psychostimulants(methamphetamine, cocaine). In other words, mGluR5-null phenotype do not exhibit opioid or cocaine induced conditional place preference. Correct me if I am wrong!!
My question is: do opioids and psychostimulants also produce "euphoria" and other NAcc mediated effects of OPs/STIMS in mGluR5-null mice without the reinforcing present in the wild-type mice? If that would be the case, then would addition of a mGluR5 antagonist to an opiate or a stim provide both potentiation of Nacc-mediated "reward" effect of OP and Stims without the reinforcing??
MGluR5, iirc is also involved in memory consolidation, learning and perception. So the question is: does mGluR5 antagonism prevent the consolidation ot the "memory of the experience" of euphoria associated with Nacc DAergic activation? So the brain can still have good time but don't make such a big deal out of it?? Much like a computer without a "SAVE" button, the "experience" of OP or Stim is just not saved. So every time you experience OP or Stim would be exactly like the last time? the last brain configuration so to speak!
If that was the case, you could then potentially design opioids and/or stimulants devoid of reinforcing effect ie selective mu agonist+MGluR5 antagonist? like a non-reinforcing fentanyl?? but then again, Would there even be "euphoria" if the experience can't be remembered by virtue of blocking type 5 Glutamate metabotropic receptors in the Nucleus accumbens??...
My question is: do opioids and psychostimulants also produce "euphoria" and other NAcc mediated effects of OPs/STIMS in mGluR5-null mice without the reinforcing present in the wild-type mice? If that would be the case, then would addition of a mGluR5 antagonist to an opiate or a stim provide both potentiation of Nacc-mediated "reward" effect of OP and Stims without the reinforcing??
MGluR5, iirc is also involved in memory consolidation, learning and perception. So the question is: does mGluR5 antagonism prevent the consolidation ot the "memory of the experience" of euphoria associated with Nacc DAergic activation? So the brain can still have good time but don't make such a big deal out of it?? Much like a computer without a "SAVE" button, the "experience" of OP or Stim is just not saved. So every time you experience OP or Stim would be exactly like the last time? the last brain configuration so to speak!
If that was the case, you could then potentially design opioids and/or stimulants devoid of reinforcing effect ie selective mu agonist+MGluR5 antagonist? like a non-reinforcing fentanyl?? but then again, Would there even be "euphoria" if the experience can't be remembered by virtue of blocking type 5 Glutamate metabotropic receptors in the Nucleus accumbens??...
With stimulants:Blockade of mGluR5 in the nucleus accumbens shell but not core attenuates heroin seeking behavior in rats
Aim:
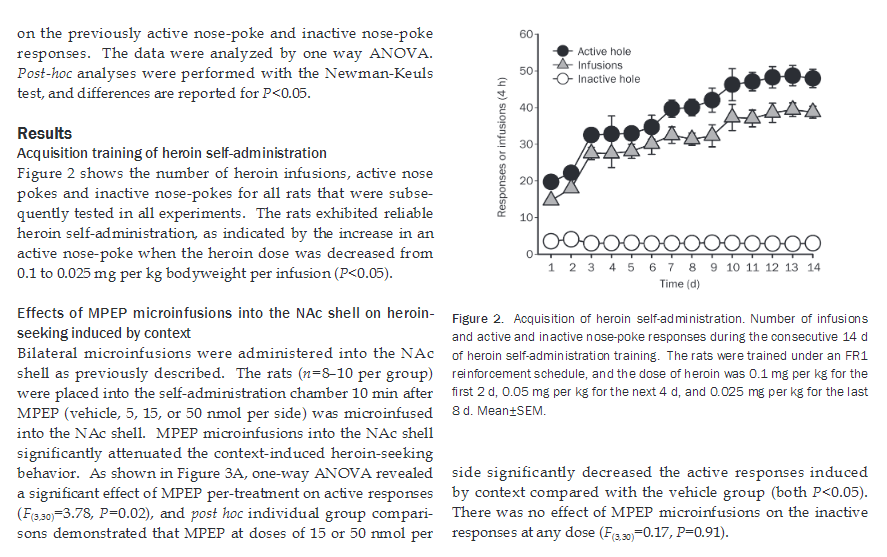
Glutamatergic neurotransmission in the nucleus accumbens (NAc) is crucial for the relapse to heroin seeking. The aim of this study was to determine whether mGluR5 in the NAc core or shell involved in heroin seeking behavior in rats.
Methods:
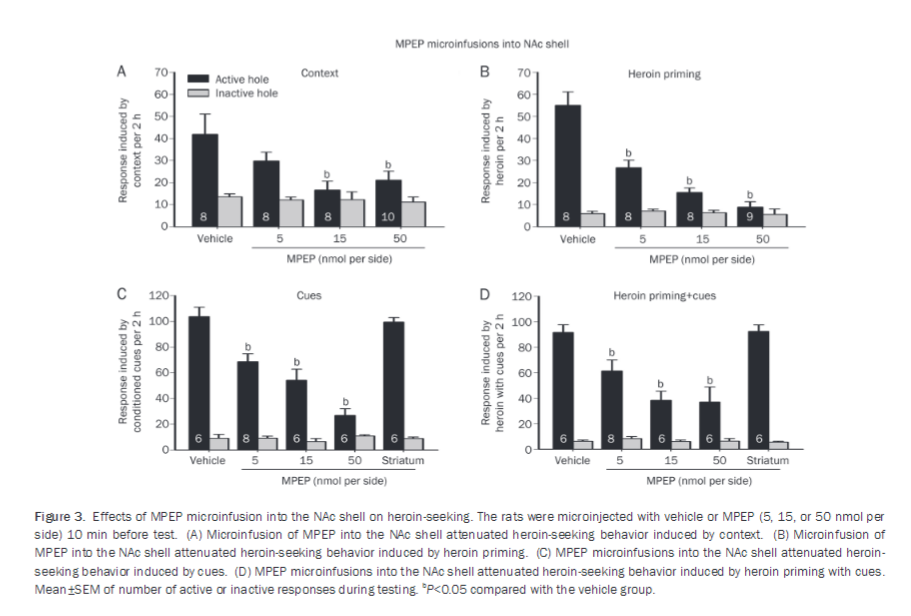
Male SD rats were self-administered heroin under a fixed-ratio 1 (FR1) reinforcement schedule for 14 d, and subsequently withdrawn for 2 weeks. The selective mGluR5 antagonist 2-methyl-6-phenylethynyl-pyridine (MPEP, 5, 15 and 50 nmol per side) was then microinjected into the NAc core or shell 10 min before a heroin-seeking test induced by context, cues or heroin priming.
Results:
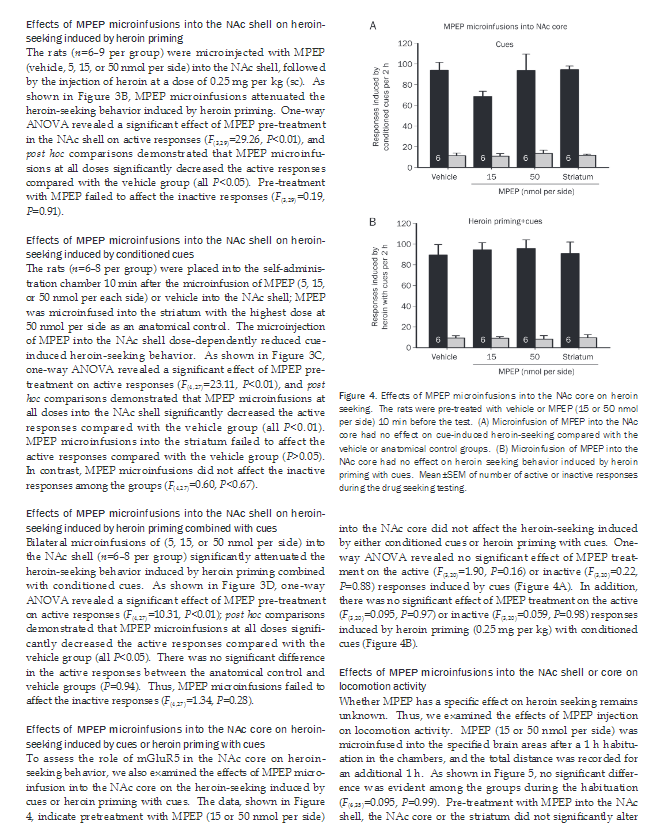
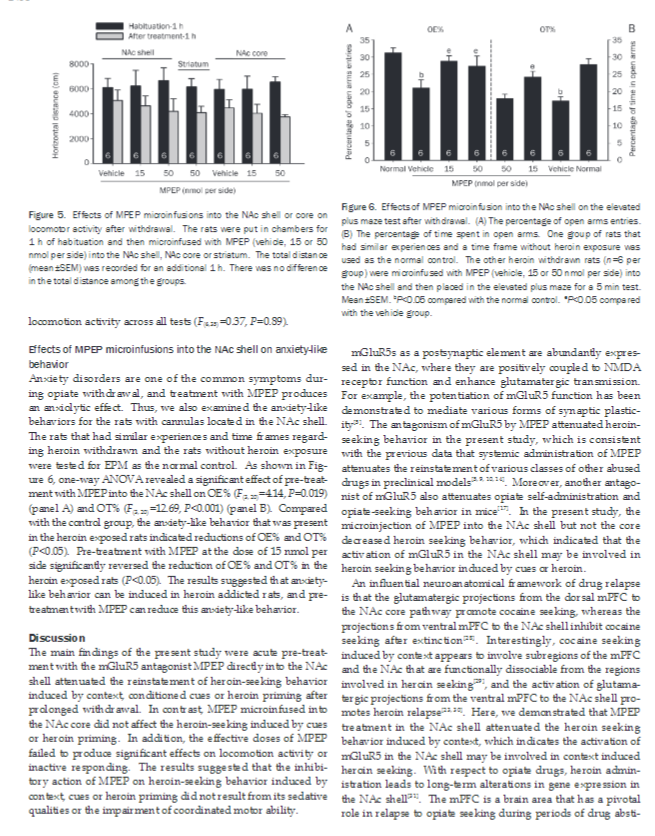
Microinjection of MPEP into the NAc shell dose-dependently decreased the heroin seeking induced by context, cues or heroin priming. In contrast, microinjection of MPEP into the NAc core did not alter the heroin seeking induced by cues or heroin priming. In addition, microinjection with MPEP (15 nmol per side) in the NAc shell reversed both the percentage of open arms entries (OE%) and the percentage of time spent in open arms (OT%) after heroin withdrawal. Microinjection of MPEP (50 nmol per side) in the striatum as a control location did not affect the heroin seeking behavior. Microinjection of MPEP in the 3 locations did not change the locomotion activities.
Conclusion:
Blockade of mGluR5 in NAc shell in rats specifically suppresses the relapse to heroin-seeking and anxiety-like behavior, suggesting that mGluR5 antagonists may be a potential candidate for the therapy of heroin addiction.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4261128/
A Novel mGluR5 Antagonist, MFZ 10-7, Inhibits Cocaine-Taking and Cocaine-Seeking Behavior in Rats
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3942387/


") ). And they get pretty excited on coke or Meth! They just don't give a hoot about doing the drug again. My guess is mGluR5 is probably not involved in short term memory formation. But only in long term potentiation (I'll have to do some more reading on that).
). And they get pretty excited on coke or Meth! They just don't give a hoot about doing the drug again. My guess is mGluR5 is probably not involved in short term memory formation. But only in long term potentiation (I'll have to do some more reading on that).