Just relax man. There's no reason to get all hot and bothered.
You are right and I am wrong on this. But if you WANT to learn, people really will help you. People who hold formal qualifications in medicinal chemistry and the occasional autodidacts like sekio (whose knowledge is very impressive) are here. The guys who came up with MXE, U-47700 (and U-47783), pyrazolam, MDPV, diclazepam and many others all view quite regularly. I'm sure a lot of others have developed other things are also here but don't mention it.
Image 1 hosted in ImgBB

ibb.co
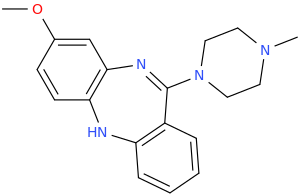
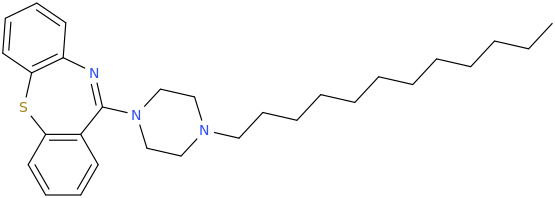
If you read about both you will notice that clozapine has many metabolic pathways but actually a shorter T1/2. The design of olanzapine has that 2-methyl on the thiophene ring. This is termed a 'sacrificial moiety'. It increases activity (directly and by increasing LogP) AND gives the body a single, simple way to metabolize the compound, Clozapine's -Cl was likewise introduced to increase potency (and does increase T1/2) but even with the sacrificial moiety, olanzapine is not only more potent but has a longer duration. Evidently an enzyme capable of oxidizing it isn't too common in the brain (more common in the body). Chlorine is most commonly chosen as it's the least toxic to the body so if a halide-exchange were to somehow take place, it would almost always be one -Cl being swapped for another -Cl. The body uses -Cl in lots of transmitters whereas -Br and -I are used but in tiny amounts. Of course, -F is so chemically inert that it's the best option 'when size doesn't matter'.
Both medicines are VERY dirty but the 'magic' of clozapine that made it so successful was that it effectively treated refractive patients. Just why wasn't appreciated until the NMDA hypothesis became popular.
Their IS a medical test for schizophrenia. It was discovered that the cerebrospinal fluid of suffers either had elevated levels of DOPAC (a dopamine metabolite) and/or reduced levels of NMDA. I think something like 80% of suffers have elevated DOPAC, 10% have lowered NMDA and 10% have both features.
So from about 2000 two groups set out to develop novel compounds to normalize the levels of NMDA. IN that 10% these drugs worked with almost no side-effects whatsoever. It was hoped that the elevated DOPAC was a result of NMDA inhibition but this proved no to be the case, After 14 years of work and trials involving hundreds of patients, these new classes were dumped because they were only effective for a minority of patients... and I'm sure you can guess which ones.
It's a really sad story because it would appant that schizophrenia actually has 2 physiological causes but a drug only useful for refractive patients... and only a proportion of those (some with low NMDA also have increased DOPAC). I would have introduced it along with the cerebrospinal fluid study being part of the diagnosis but unless you have a blockbuster, you would end up losing money by making it available. To be fair, they are now termed 'orphan drugs' i.e. patent rights have been waived.
Schizophrenia is also a very unusual disease because while it does have a strong genetic basis, only 50% of identical twins (monozygotic) will both develop the illness. That's because even though we use the term 'identical', the DNA is not in fact identical.
As we age our DNA changes and even that which is the same may undergo epigenetic changes (parts are switched on or off). This is likely why their it an equally important nurture element. It seems to have existed for as long as written history but the attitude of the general public has altered considerably. Until about 300 years ago it was believed that suffers were closer to god and were supported within communities.
But when medicine classified it as a disease, it was pathologized and suffers were segregated. In my opinion, the most important book on the topic is 'The History of Madness' (originally translated as 'Madness and Civilization) by the French philosopher Michel Foucault. He examines attitudes from the middle ages until (almost) modern times (first published in 1961).
It was the beginning of effective neuroleptics becoming available and the reintegration of those with the illness but who benefit from medication and he explores the possible futures. Of course, in 1961 the serious and often irreversible side-effects of neuroleptics wasn't as well known.
My interest is because a school friend developed schizophrenia in his mid 20s. As you might know, late onset is generally harder to treat. It didn't all happen at once and being younger than him, I didn't know what to make of it. What I DO know is that he lost his job, his GF left him and his dog died all within a span of 2 weeks. A trigger event if you will.
He started to believe I was Satan and had done all kinds of nasty things to him like make his friends avoid him. I had to get a restraining order.
He got very sick indeed. In the end he hired a car, drove to France, maxed out his credit card and when he came back into the UK he tried to use the card to fill up with fuel. The assistant seized the card (he had spent almost £20000 and his limit was £3000). He leapt over the counter and almost beat the assistant to death.
Of course he was arrested but within 12 hours he had been moved to an RSU (regional secure unit) and I'm sorry to say he ended up in Rampton for a while.
He was medicated but the last I heard of him was in 2001 when he tried to burn down his home. NOW I would know. NOW I would have some insights but back then I knew no medicinal chemistry or ANYTHING about schizophrenia.