RoboRobot
Bluelighter
- Joined
- Aug 26, 2009
- Messages
- 58
So, I was looking into nasal anatomy to see where would be the best place to try and "direct" the powder I am insufflating into my nostril (or liquid solution). It seems from experience that you can snort too hard, and it'll go to the back of the throat, or too little and powder will fall out. (Usually never have these issues, but still curious.) So, I wanted to look into the best place to position the straw or oral syringe to place either powder, or liquid solution, in the most efficient place in my nasal cavity.
I did a bit of research and I'll post some quotes and links and images of what I've found. (PS- if you'd like to look at a few images beforehand so you can clearly picture what Im talking about, scroll down and open up the spoiler tags- they contain illustrations of the nasal anatomy.)
So, basically, there seems to be the three separate sections in the nose that have the ability to absorb a drug due to it's mucus membrane. They're called turbinates. There's the lower "inferior" turbinate, middle turbinate, and upper "superior" turbinate.
Here's some explanation:
Justin H. Turner, M.D., Ph.D.
Devyani Lal, MD
Jayakar V. Nayak, MD, PhD
http://care.american-rhinologic.org/nasal_anatomy?print
And here's the physiology: http://care.american-rhinologic.org/nasal_physiology
(Me again :D haha) So, basically what I deduced from that is it seems the lower (inferior) turbinate would have the best absorption rate, due to it's larger surface area and being the most vascular of the three (the veins being necessary to absorb any drug in the membrane).
Here's a quote from the same three doctors on the blood supply in the nose:



^^^ Those pictures I wrapped in spoiler tags so they wouldnt have to load if people didnt feel like looking at them. I am unsure if I should've done this or if this is the way to do it, so please let me know if I need to change something. These pictures are just illustrations, nothing graphic at all, just to let you know.
Anyways, judging by those pictures, I can almost imagine an exact position of the straw (or oral syringe w/ solution) during intranasal use to get the majority into the lower turbinate.. It seems to be helpful information to know if you insufflate anything. I know I was always worried about it not getting to the best possible place in my nose and getting wasted, and I like being informed on what drugs do to my body and how.
So, I thought it was far past the due time for me to figure this out, and Ill be a lot more comfortable next time I insufflate knowing Im not just going off what people say on the street. (e.g. vitamin c helps mdma, lsd stored in spine, lololol etc)
I wanted this to remain as professional and informative as possible, but alas, I am not 100% *positive* on my conclusion. I would really enjoy any opinions on the matter, or better yet, any supporting factual data! Is the lower turbinate the best for absorption due to the highest amount of capillaries and veins? Seems plausible, but Im not well-versed in Nasal Anatomy
Would love to see the discussion start flowing, though. It'd help us get better BA intranasally if we actually had an exact planned destination for said insufflated substance.
!!!!
oh yeah, and judging by my first quote, where they are talking about lateral sidewalls (and adjacent mucus membrane) makes me almost think that these turbinates are located on the SIDES of the nose. But judging by the pictures, these turbinates look to clearly run horizontally, not vertically.
As quoted from the article the lower turbinate "runs along the entire length of the lateral nasal wall, adjacent to the nasal floor."
I was initially planning to try and direct insufflated material to just a tiny bit above the floor of my nasal cavity, where the pictures seem to show the lower turbinate. Reading that quote makes me think otherwise, though, and maybe it'd be better to position it towards the side walls of my lower nasal cavity. Any info on the matter would be greatly appreciated!
(here's some illustrations I just pulled up of the "lateral" nose walls and turbinates.. Let's see what you guys can make of it %) )
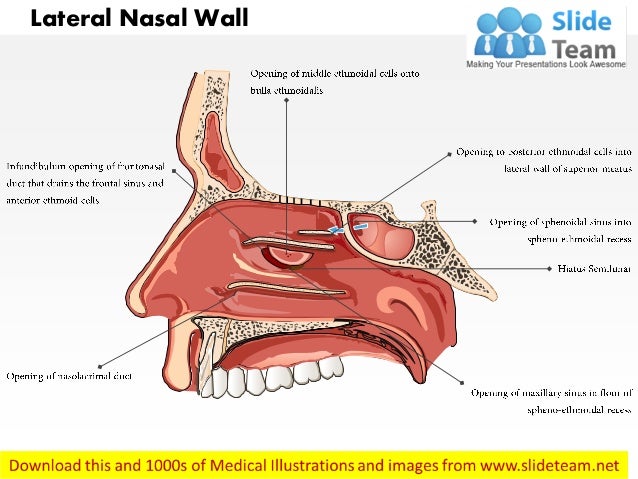
http://www.instantanatomy.net/diagrams/HN075b.png[IMG]
[IMG]http://image.slidesharecdn.com/lec-140909023023-phpapp01/95/lec4nose-ptrc-7-638.jpg?cb=1410229896
lat·er·al
ˈladərəl,ˈlatrəl/
adjective
1.
of, at, toward, or from the side or sides.
"the plant takes up water through its lateral roots"
synonyms: sideways, sidewise, sideward, edgewise, edgeways, oblique, horizontal
"lateral movements"
noun
1.
a side part of something, especially a shoot or branch growing out from the side of a stem.
but this still throws me off: lower turbinate "runs along the entire length of the lateral nasal wall, adjacent to the nasal floor." Right when I think I have it all figured out. I have a pretty good idea, just would love some feedback!
I did a bit of research and I'll post some quotes and links and images of what I've found. (PS- if you'd like to look at a few images beforehand so you can clearly picture what Im talking about, scroll down and open up the spoiler tags- they contain illustrations of the nasal anatomy.)
So, basically, there seems to be the three separate sections in the nose that have the ability to absorb a drug due to it's mucus membrane. They're called turbinates. There's the lower "inferior" turbinate, middle turbinate, and upper "superior" turbinate.
Here's some explanation:
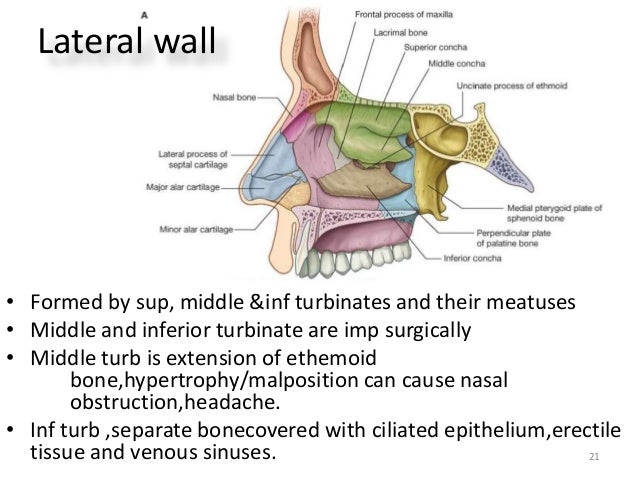
"The nasal cavity is bounded in by bony sidewalls (lateral nasal walls). Attached to these sidewalls are three structures called turbinates. The turbinates are fingerlike projections made up of a bony core and outer soft tissue. They are covered with a lining (mucosa) which is continuous with the lining of the rest of the nasal cavity. The turbinates serve to increase the mucosal surface area of the nasal cavity, and also direct smooth nasal airflow towards the lungs. Between each turbinate and nasal sidewall lies a space termed a meatus. These spaces are named according to the turbinate above them.
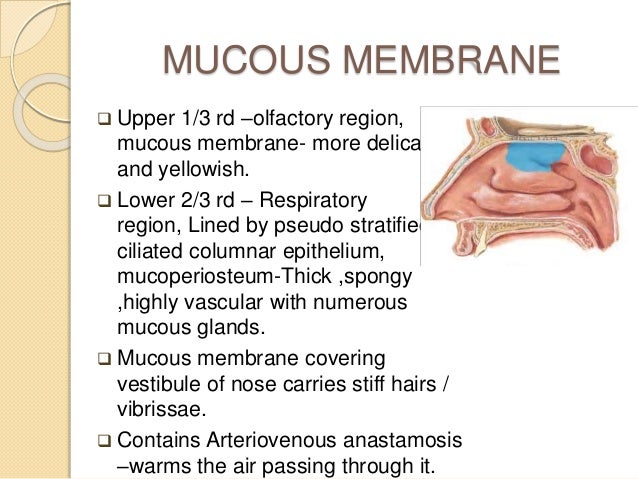
The bottom most turbinate, the “inferior” turbinate serves the most important role in the air-conditioning action of the nose. This capacity of the inferior turbinate comes from soft tissue below the lining. This tissue is extremely rich in blood vessels and glands, and helps the nasal air-conditioning function. The inferior turbinate is the largest of the three paired turbinates, and runs along the entire length of the lateral nasal wall, adjacent to the nasal floor. Sometimes, the inferior turbinate can get enlarged due to allergy or irritation, and can cause nasal blockage and a runny nose. The tear duct (nasolacrimal duct), which drains tears from the eye, drains beneath the inferior turbinate into the inferior meatus.
The middle turbinate lies above the inferior turbinate and is a very important structure with a complex, boomerang shape. The front part of the middle turbinate is vertical, attaching to the skull base. The back of the middle turbinate is horizontal, and attaches to the nasal sidewall just above the inferior turbinate. The middle part of the middle turbinate is oblique, connecting the vertical and horizontal parts, and is thus connected both the skull base in the front and the nasal sidewall in the back. The frontal sinus and anterior ethmoid sinus cells drain beneath the middle turbinate into the middle meatus.
The superior turbinate is the smallest of the turbinates. It resides just above and behind the middle turbinate. The sphenoid sinus and posterior ethmoid sinus cells drain into an area between the nasal septum and superior turbinate called the sphenoethmoid recess."
Justin H. Turner, M.D., Ph.D.
Devyani Lal, MD
Jayakar V. Nayak, MD, PhD
http://care.american-rhinologic.org/nasal_anatomy?print
And here's the physiology: http://care.american-rhinologic.org/nasal_physiology
(Me again :D haha) So, basically what I deduced from that is it seems the lower (inferior) turbinate would have the best absorption rate, due to it's larger surface area and being the most vascular of the three (the veins being necessary to absorb any drug in the membrane).
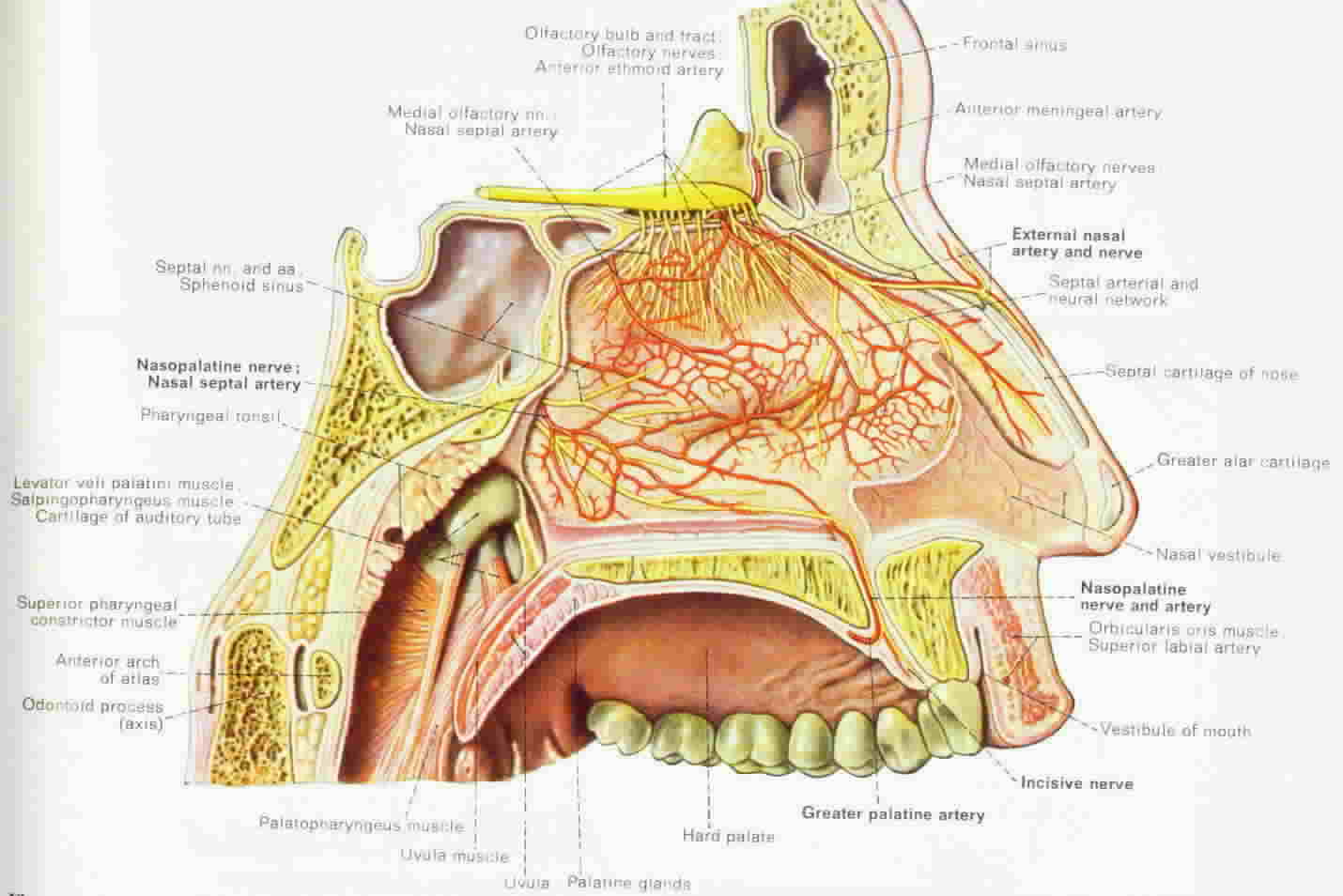
Here's a quote from the same three doctors on the blood supply in the nose:
BLOOD SUPPLY
"The nasal cavity has a very rich blood supply arising from both the internal and external carotid arteries. A confluence of these blood vessels supplying the nasal septum in the front (“Kiesselbach plexus” in the “Little’s area”) is a common source of nasal bleeding (epistaxis). This area can often be cauterized in the office to stop nasal bleeding. The anterior and posterior ethmoid arteries, both branches of the internal carotid artery system supply the upper nasal septum and nasal sidewalls. The superior labial branch of the facial artery supplies the front part of the nose. The sphenopalatine artery, a branch of the external carotid system supplies most of the back of the nasal cavity. It enters the nasal cavity through an opening located along the nasal sidewall called the sphenopalatine foramen. When nasal bleeding is more from the back part (posterior epistaxis), this artery is often the culprit. When recurrent posterior epistaxis becomes a problem, the sphenopalatine artery may need to be tied or embolized.
In addition to this larger vasculature, there is a confluence of the small vessels that supplythe front portion of the nasal septum that is termed Kiesselbach’s plexus. This lattice of veins is a common source of nasal bleeding (epistaxis) due to trauma and dry air exposure, and may require medical attention in many cases."
^^^ Those pictures I wrapped in spoiler tags so they wouldnt have to load if people didnt feel like looking at them. I am unsure if I should've done this or if this is the way to do it, so please let me know if I need to change something. These pictures are just illustrations, nothing graphic at all, just to let you know.
Anyways, judging by those pictures, I can almost imagine an exact position of the straw (or oral syringe w/ solution) during intranasal use to get the majority into the lower turbinate.. It seems to be helpful information to know if you insufflate anything. I know I was always worried about it not getting to the best possible place in my nose and getting wasted, and I like being informed on what drugs do to my body and how.
So, I thought it was far past the due time for me to figure this out, and Ill be a lot more comfortable next time I insufflate knowing Im not just going off what people say on the street. (e.g. vitamin c helps mdma, lsd stored in spine, lololol etc)
I wanted this to remain as professional and informative as possible, but alas, I am not 100% *positive* on my conclusion. I would really enjoy any opinions on the matter, or better yet, any supporting factual data! Is the lower turbinate the best for absorption due to the highest amount of capillaries and veins? Seems plausible, but Im not well-versed in Nasal Anatomy
Would love to see the discussion start flowing, though. It'd help us get better BA intranasally if we actually had an exact planned destination for said insufflated substance.
!!!!
oh yeah, and judging by my first quote, where they are talking about lateral sidewalls (and adjacent mucus membrane) makes me almost think that these turbinates are located on the SIDES of the nose. But judging by the pictures, these turbinates look to clearly run horizontally, not vertically.
As quoted from the article the lower turbinate "runs along the entire length of the lateral nasal wall, adjacent to the nasal floor."
I was initially planning to try and direct insufflated material to just a tiny bit above the floor of my nasal cavity, where the pictures seem to show the lower turbinate. Reading that quote makes me think otherwise, though, and maybe it'd be better to position it towards the side walls of my lower nasal cavity. Any info on the matter would be greatly appreciated!
(here's some illustrations I just pulled up of the "lateral" nose walls and turbinates.. Let's see what you guys can make of it %) )
http://www.instantanatomy.net/diagrams/HN075b.png[IMG]
[IMG]http://image.slidesharecdn.com/lec-140909023023-phpapp01/95/lec4nose-ptrc-7-638.jpg?cb=1410229896
lat·er·al
ˈladərəl,ˈlatrəl/
adjective
1.
of, at, toward, or from the side or sides.
"the plant takes up water through its lateral roots"
synonyms: sideways, sidewise, sideward, edgewise, edgeways, oblique, horizontal
"lateral movements"
noun
1.
a side part of something, especially a shoot or branch growing out from the side of a stem.
but this still throws me off: lower turbinate "runs along the entire length of the lateral nasal wall, adjacent to the nasal floor." Right when I think I have it all figured out. I have a pretty good idea, just would love some feedback!
Last edited:

 ) has a far higher solubility in alcohol versus water. So, with the added benefit of it being more soluble in alcohol, it will also dilate my blood vessels thus enabling quicker absorption of a *more concentrated* (and thus more potent) solution of said opioid.
) has a far higher solubility in alcohol versus water. So, with the added benefit of it being more soluble in alcohol, it will also dilate my blood vessels thus enabling quicker absorption of a *more concentrated* (and thus more potent) solution of said opioid.")