AlsoTapered
Bluelighter
- Joined
- Apr 1, 2023
- Messages
- 3,076
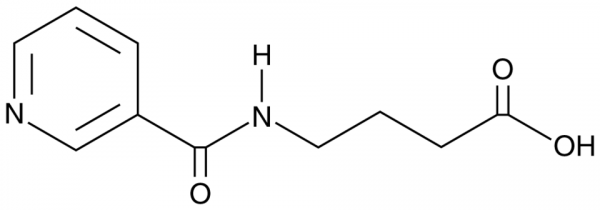
No - hydrolysis will leave nicotinamide and a hydroxyl moiety as picamilon does.
N&PD Moderators: Skorpio | thegreenhand





It may be worth your time to watch (or indeed read the original book) 'The Case of the Frozen Addicts'.
Near the end it was suggested that in the future an MRI scan would detect those likely to develop Alzheimer's and those who were at risk would simply be prescribed meclobemide (if memory serves) which is an MAOI.
It's interesting that centrophenoxine displays MAO activity and is structurally similar to meclobemide.
Now, that 'future' never happened. I don't know why.
But it does seem that maintaining neuroplasticity is an important defence. People with quite advanced forms of dementia (from a structural point of view) who maintain patterns of learning do appear to survive and more importantly remain mentally aware for longer.
Someone I know has serious fear for Alzheimer. Age 67 (she has skin Lupus to), another family member is 96 (cognitively still ok) but IMO also a good candidate.
At 50 my own body is showing Liverspot's, so I'll experiment on myself too.
To bad Centrophenoxine is not used by dr's over here, its not mentioned in their drug bible like many nootropic's.
The Lipofuscin removal/ anti Alzheimer effect do they still stand or has that been proven wrong. Anyone knows? I did search, but you are my knowledge database.
Is it worth to try, the fact its for someone else worries me as I ain't no dr. and never took it.
Should they tell there dr's. Has it interaction's with prescription medication's that you must be beware of.
 swisstargetprediction.ch
swisstargetprediction.ch
"The case of the Frozen Addict's" is that a book you'll find in a library? Bizar title btw. Thanks for the pointer.It may be worth your time to watch (or indeed read the original book) 'The Case of the Frozen Addicts'.
Near the end it was suggested that in the future an MRI scan would detect those likely to develop Alzheimer's and those who were at risk would simply be prescribed meclobemide (if memory serves) which is an MAOI.
It's interesting that centrophenoxine displays MAO activity and is structurally similar to meclobemide.
Now, that 'future' never happened. I don't know why.
But it does seem that maintaining neuroplasticity is an important defence. People with quite advanced forms of dementia (from a structural point of view) who maintain patterns of learning do appear to survive and more importantly remain mentally aware for longer.
Meclobemide, assuming you mean Moclobemide the MAO-inhibitor prescription anti depressant, in other word's fat chance they will be able to get it. Way to many side effect's and interaction's and which dr. would be prepared I wonder.
But the Centrophenoxine is not for me so that's another story. I take L-Acetyl-Carnitine to repair my Hippocampus. Centrophenoxine is contradicted for Epileptic's.